Background: Stony Brook University Hospital (SBUH) identified an opportunity to develop and implement prevention strategies to reduce hospital onset C. difficile infections (CDI). Hospital Onset (HO) CDI are included in National Healthcare Safety Network (NHSN) reporting and included with other hospital-acquired infections as publically reported data. CDI contribute to prolonged hospital stays, inappropriate antimicrobial use, increased readmissions, and high costs for any institution. A Quality Improvement (QI) team was tasked to focus on decreasing HO CDI in early 2016 and included a multidisciplinary team with departmental representatives from Executive leadership, Healthcare Epidemiology, Nursing, Quality Improvement, Hospitalist, Infectious Disease and Laboratory staff. A gap analysis of the variance between ourcurrent and future states, based on best-practice guidelines from CDC and Society for Healthcare Epidemiology of America (SHEA), provided multiple avenues of opportunity to focus our efforts, including IT guardrails, a robust education initiative, an antimicrobial stewardship program, and room turnover cleanliness compliance.
Purpose: Through small tests of change, the team will implement rigorous Plan-Do-Check-Act (PDCA) cycles throughout 2016 to evaluate their efficacy, functionality and
contribution to decreasing HO CDI and optimizing patient outcomes. By 2017, the goals include:
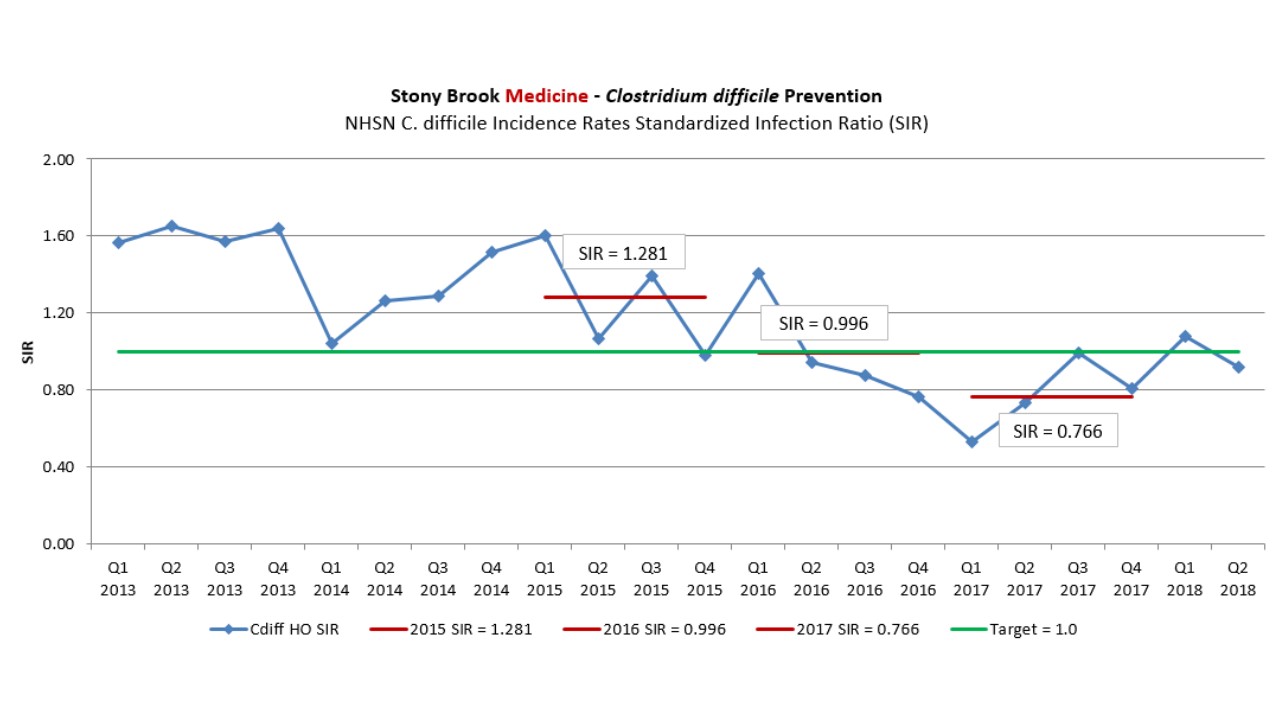
1) Decrease HO CDI Standardized Infection Ratio (SIR) <1.0 with a stretch goal of 0.8
2) Reduce hospital onset C. difficile (CD) infection rates by 20% from 2015 rate
3) Implement the CD Information Technology (IT) Tableau reporting dashboard for real-time tracking of unit and physician specific test ordering
4) Develop a comprehensive CD prevention education program
Description: Historic data showed testing was over-utilized and often revealed patients with colonization, rather than a true infection. CDC and SHEA guidelines recommend testing only patients with select risk factors, signs and symptoms consistent with CDI, with no use of laxatives within 48 hours, and with three diarrheal stools documented within 24 hours. An Electronic Medical Record (EMR) alert was designed and tested throughout 2016 to automatically review records for these criteria with an order for CD testing. If such evidence was found, the EMR would
lock out all house staff orders with a reminder that CDC guidelines advise against such testing. Attending physicians would also receive this alert, but with the distinct ability to bypass based on a patient’s clinical presentation. Reports were designed to discover HO CDI in as real-time as possible in order to review and report on the root causes of each case in a timely manner, as well as
developing monthly and quarterly trend reports to track unit order volumes, HO CDI rates, and our NHSN Standardized Infection Ratio (SIR). The IT department developed reporting software through Cerner EMR HealtheIntent. This CD dashboard provides hourly refreshed reporting for all positive testing.Using Root Cause Analyses (RCA) case reviews from the Healthcare Epidemiology Department (HED) and monthly analysis of alert bypass volumes,the team was able to evaluate and respond to each HO-CDI case and relay any opportunities to pertinent nursing and physician staff.
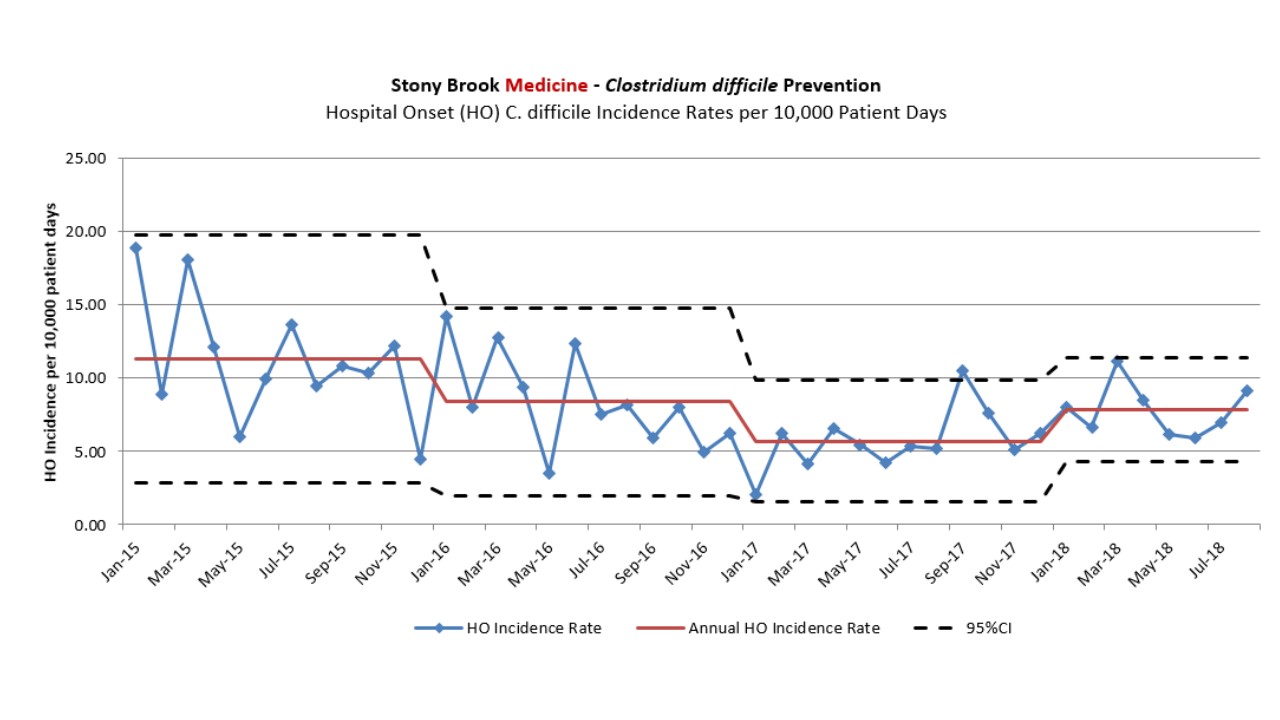
Conclusions: -Rate of HO CDI Incidence per 10,000 patient days decreased 49.5% from 11.3 in 2015 to 5.7 in 2016
-NHSN SIR decreased throughout the year, achieving 0.993 for 2016 and below the stretch goal for 2017, 0.766