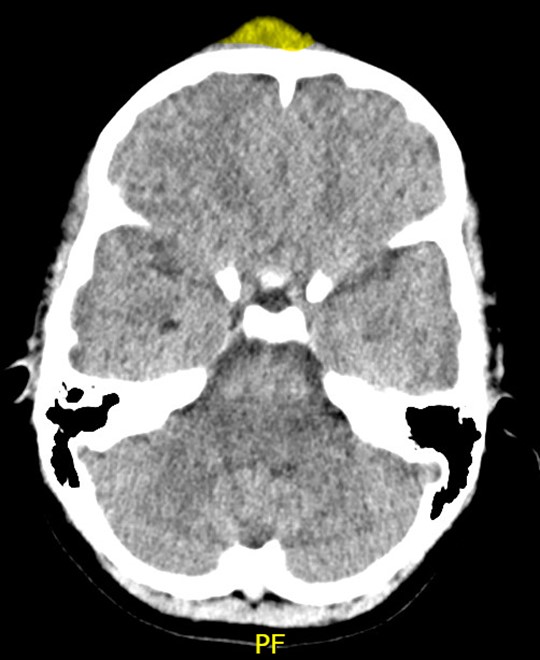
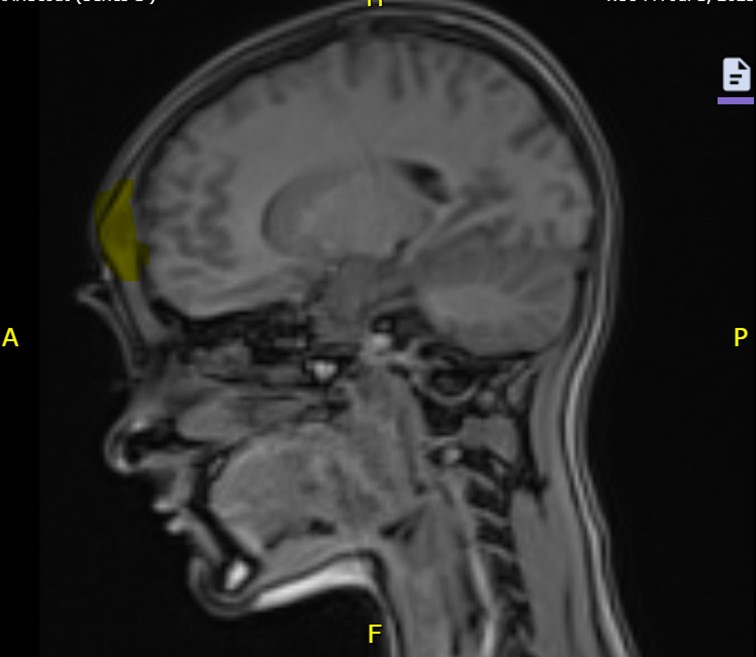
Case Presentation: A 12-year-old female presented to the ED with 14 days of progressive forehead swelling following treatment for sinusitis and conjunctivitis. Four weeks earlier, she sought medical attention for forehead swelling and headache and completed a 10-day course of amoxicillin-clavulanate for left eye conjunctivitis and frontal sinusitis, with resolution of symptoms. 2 days prior to ED presentation her forehead swelling recurred following mild head trauma. In the ED, she was noted to have a mildly tender 4×4 cm area of induration over her forehead. Non-contrast head CT showed frontal scalp induration with mottling of the underlying frontal bone, outer table thinning, and bony changes extending toward the frontal sinus. Findings suggested an early subperiosteal abscess of the frontal bone (Pott’s Puffy Tumor), and she was hospitalized.MRI of the brain demonstrated extensive sinus inflammation, an extracranial abscess overlying the anterior calvarium, and frontal bone erosion. Otolaryngology (ENT), Neurosurgery, and Infectious Disease (ID) were consulted, and she was treated with ceftriaxone, metronidazole, and vancomycin. A bedside nasal culture grew H. influenzae and endoscopic sinus surgery cultures grew methicillin-sensitive S. aureus and S. mitis-oralis. While hospitalized, she completed 7 days of IV antibiotics following surgery and her clinical status improved. She transitioned to daily ertapenem via PICC line prior to discharge on hospital day 9 and ultimately completed a course of 4 total weeks of antibiotics.
Discussion: This case underscores the sequalae of unresolved bacterial sinusitis when compounded by minor head trauma. Subperiosteal abscesses of the frontal bone arise in the setting of acute or chronic frontal sinusitis; trauma is a risk factor that may precipitate osteomyelitis and subperiosteal abscess development. Early recognition may help prevent serious intracranial complications such as epidural abscess, subdural empyema, and meningitis (1-2).This patient’s initial forehead induration may have represented an early frontal bone subperiosteal abscess, with partial treatment by the amoxicillin – clavulanate, explaining the transient resolution before her minor trauma. Forehead induration is atypical of uncomplicated acute bacterial sinusitis and may imply complications, especially in adolescents, with frontal sinus involvement (2). Her concurrent conjunctivitis further suggests an atypical presentation and is more consistent with H. influenzae than typical acute bacterial sinusitis (3-4).Hospitalists play a pivotal role in management of frontal bone subperiosteal abscesses by providing comprehensive and timely care. Imaging confirms the diagnosis and identifies complications. Treatment begins with empirical broad-spectrum IV antibiotics to cover Streptococcus, Staphylococcus, and anaerobic organisms. Surgical and medical consultations, including ENT, neurosurgery, and ID, guide operative and antimicrobial management. Clinical status, with careful attention to pain and neurological changes, is closely monitored to assess complications.
Conclusions: Forehead induration in the context of recent sinusitis and head trauma, should lead clinicians to maintain a high index of suspicion for subperiosteal abscess of the frontal bone or Pott’s Puffy Tumor.