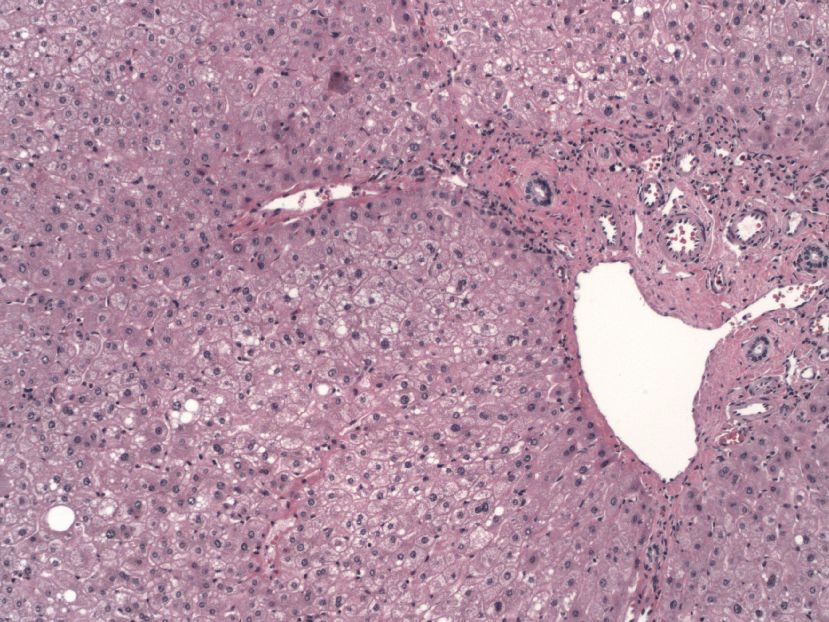
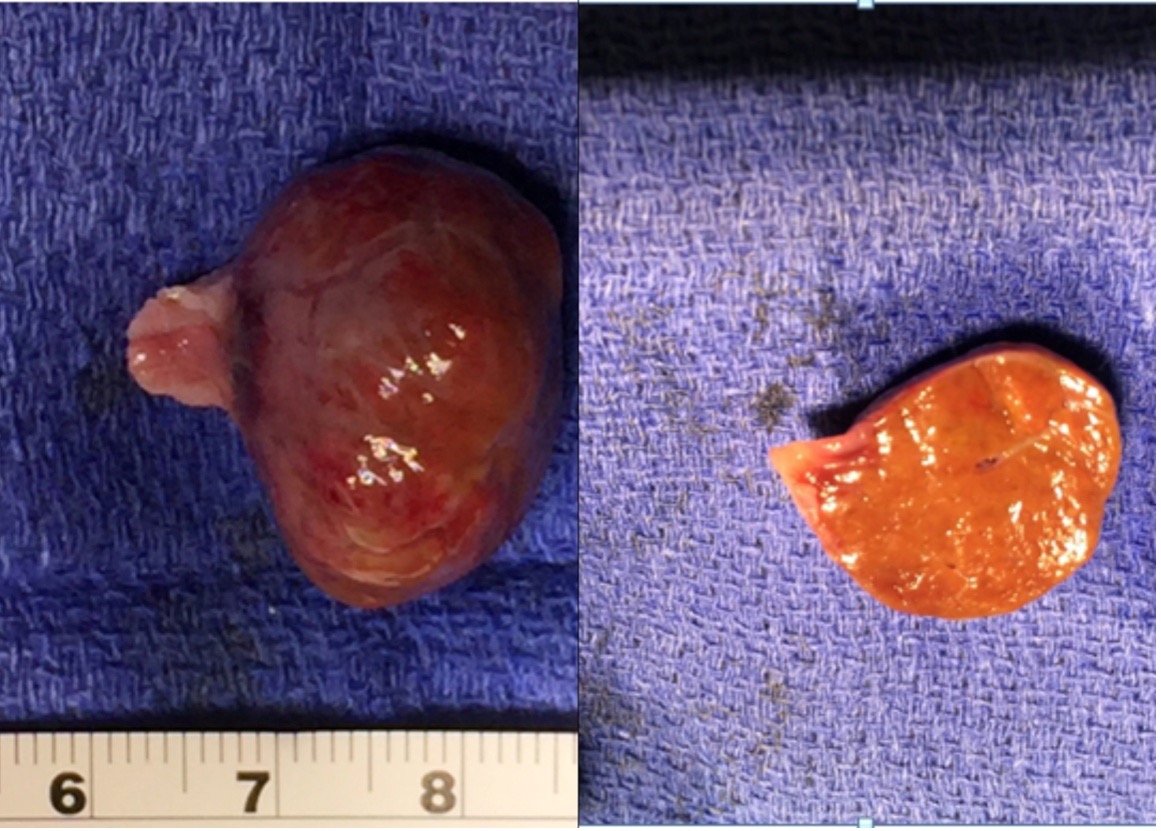
Case Presentation: Ectopic Liver is generally observed intra-abdominally, its extension supra-diaphragmatically is a rare occurrence. There are only 23 such reported cases in literature with the majority being reported in younger age groups as an extension of the caudate lobe of the liver through a diaphragmatic hernia(1,2). However, the presentation of an ectopic liver as an atrial mass in adults is an extremely rare anomaly, with only 3 reported cases in Pubmed We present the case of a 45-year-old obese Caucasian male with a history of obstructive sleep apnea who complained of worsening shortness of breath on exertion over a period of 8 months with one episode of syncope in the remote past. He denied any orthopnea, chest pain, paroxysmal nocturnal dyspnea, or lower extremity edema. Complete blood counts and metabolic panel were unremarkable. The electrocardiogram showed normal sinus rhythm. Transthoracic Echocardiogram (TTE)(Pic:1) revealed a 2.7×1.6 cm mass at the junction of the right atrium (RA) and inferior vena cava (IVC) and a patent foramen ovale(PFO) and ejection fraction of 55-60%. Cardiac surgery was consulted for resection of a presumed atrial myxoma given the possibility of embolization. A pedunculated grape-like mass of 2.9×1.8 cm of firm, brown with rubbery consistency was resected (Pic:2) followed by the closure of PFO. Histology confirmed partially encapsulated liver parenchyma. The postoperative course was unremarkable, and resolution of dyspnea was noted at follow-up.
Discussion: Right atrial masses are often an incidental discovery in echocardiography. Regardless resection often remains the default choice considering the embolic and carcinogenic potential of ectopic masses. However, there exists no imaging or diagnostic modality that can yet differentiate a cardiac tumor from an ectopic mass. A possible clue in our patient could be the location of the mass in the high IVC/RA junction. A plausible explanation for this anomaly could be the close association of liver bud, IVC, and septum transversum that allows the migration of hepatocytes into the IVC lumen during the formation of the caudate lobe.
Conclusions: The intracardiac ectopic liver is an extremely rare diagnosis, but an important one to make primarily due to an increased incidence of carcinogenesis in the ectopic tissue. In our patient, the presence of a separate tumor mass in the high inferior vena may have been a clue that this mass was not a myxoma or a renal cell carcinoma. We hope this case can serve as a good teaching point to keep broad differentials in right atrial masses instead of just fixating on a particular diagnosis