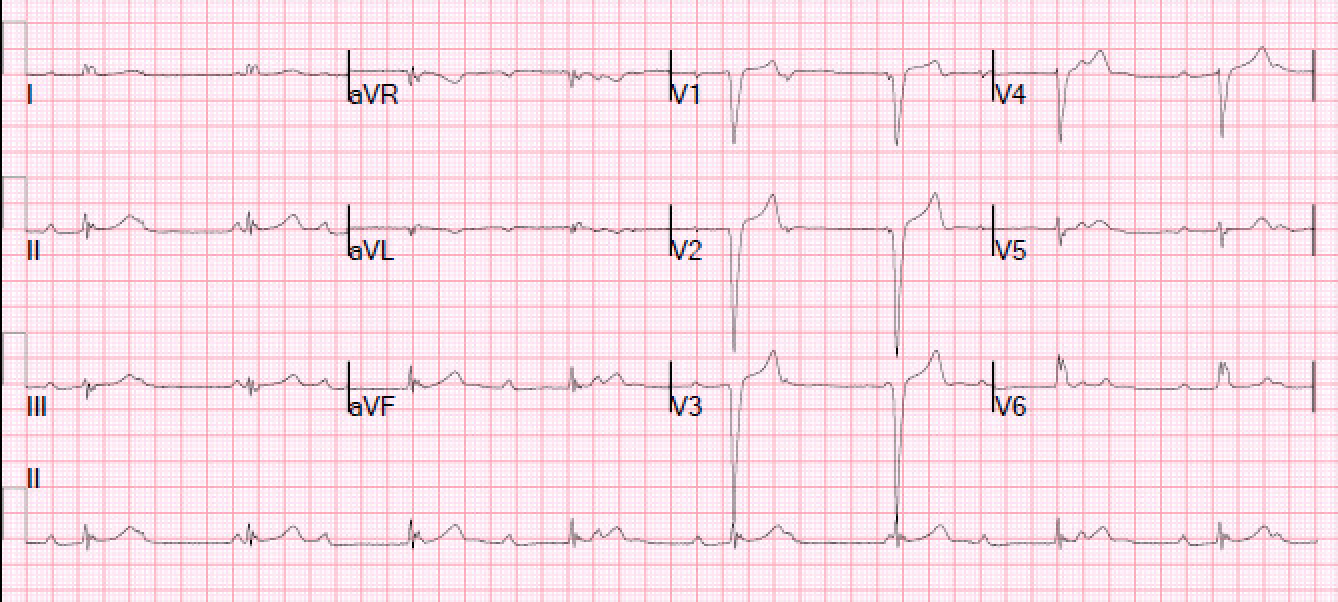
Case Presentation: A 34-year-old African American female with no significant past medical history presented to the emergency room complaining of intermittent palpitations associated with dizziness and dyspnea on exertion for six weeks. She had similar symptoms a year prior, which had resulted in a syncopal episode, however work up at that time was insignificant. Three years prior to this presentation she had been experiencing arthralgia and morning stiffness for a few months at which time she was seen by a Rheumatologist. Upon investigation she was found to have a positive ANA titer (1:1280), however her symptoms were self-limited and resolved without treatment. Upon admission she was normotensive with a blood pressure of 133/76, bradycardic with a heart rate of 50 bpm, and an unremarkable physical exam. Electrocardiogram (EKG) was significant for sinus bradycardia at 50 bpm with a first-degree Atrioventricular block, a left bundle branch block (LBBB), and QTc prolongation. A repeat EKG showed AV dissociation with an incomplete LBBB. Subsequently, further workup was performed to investigate cause of heart block. Serology was unremarkable except for high positive anti-Rho-52/SSA > 8.0 AI (<1.0). Autoimmune mediated heart block was suspected, and the patient was started on Methylprednisolone 30mg every 12 hours with complete resolution of her heart block and symptoms. She was discharged on a steroid taper and hydroxychloroquine and remained in remission on multiple outpatient follow ups therefore steroids were eventually confidently discontinued.
Discussion: Anti-Ro/SSA is one of many antinuclear antibodies; commonly seen in association with Sjogren’s syndrome (1). This specific antibody when found in women during pregnancy has been linked to both the development of congenital heart block and neonatal lupus (1). Although it has been well established that transplacental transfer of anti-Rho antibodies is associated with congenital arrhythmogenic effects in approximately 2% of babies born to SSA positive mothers, the occurrence in adults remains a rare entity. The neonatal human atrial cells differ from adult cells; the neonatal cells have a larger current density, faster inactivation, and slower recovery from inactivation; potentially explaining the association seen of Anti-Ro/SSA and congenital heart block (2). However, the exact mechanism of anti-Ro autoantibodies leading to autoimmune induced complete heart block in adult cardiac tissue remains poorly understood; as adult myocytes are resistant and autoantibody effects should be minimal and reversible.
Conclusions: This report highlights a rare case of atrioventricular heart block associated with anti-Ro/SSA antibodies in an adult, and complete resolution of conduction defect with glucocorticoids and hydroxychloroquine. The pathogenicity of anti-Ro/SSA is not completely understood; however, one proposed mechanism has been the interaction of anti-Ro antibodies with calcium channels and reversible inhibition of calcium channels (3). While the majority of cases of Anti-Ro/SSA positive conduction defects have been documented in the neonatals; complete heart block in adults related to anti-Ro autoantibodies is almost unheard of, with only a handful or reported cases worldwide. Clinicians should consider this antibody related conduction abnormality as a differential, in adults with otherwise inexplicable complete heart block.