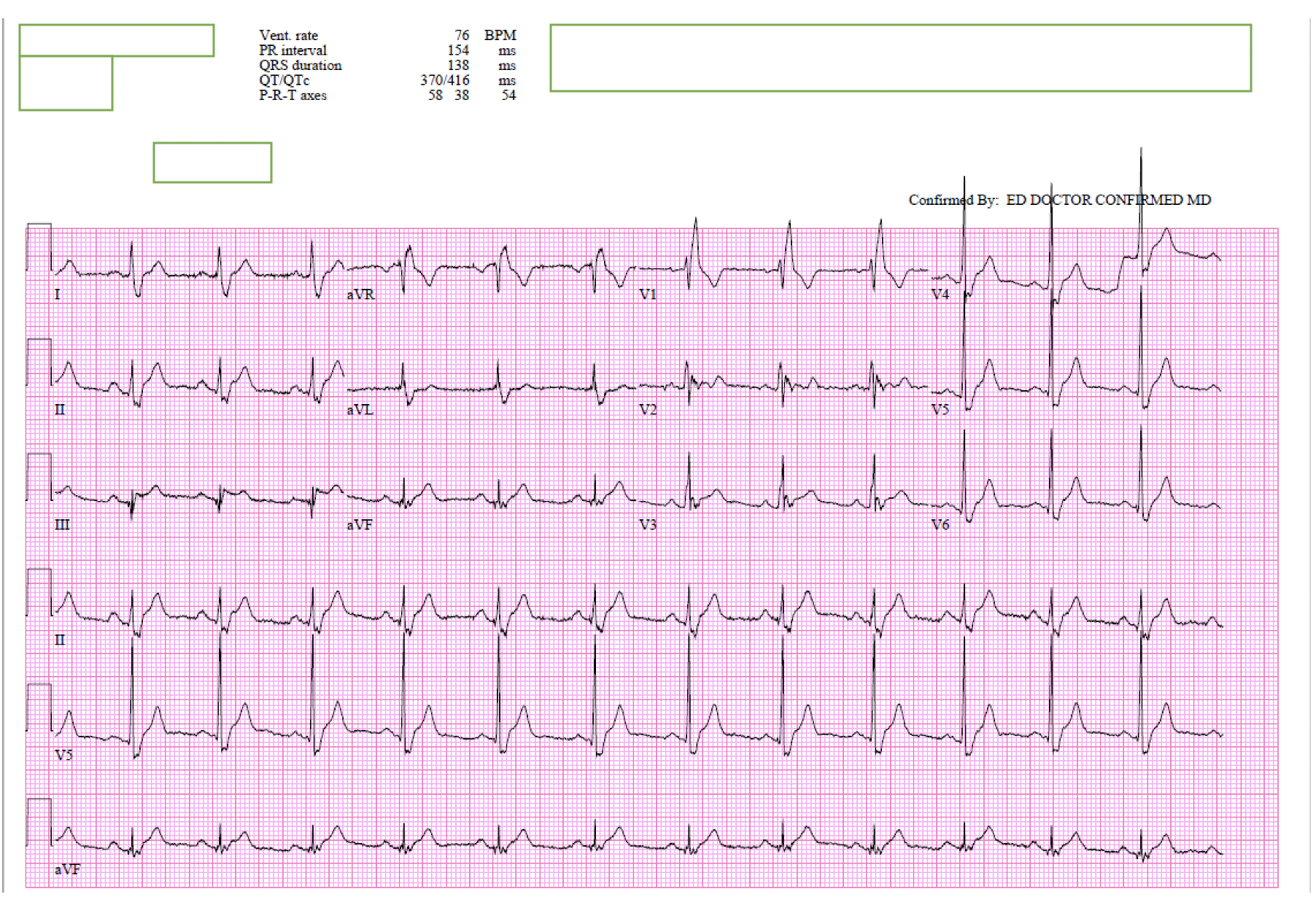
Case Presentation: Lyme disease a multisystem disease, occurring globally is caused by the spirochete borrelia burgdorferi and transmitted by the Ixodes tick.(6) The incidence of Lyme carditis (LC) is rare with reported incidences of 4%- 10% but recent studies showing 0.3% to 4% with high grade AV block is the most common presentation.(5,2) We present a case of rare simultaneous presentation of Lyme myopericarditis with erythema migrans.CASEAn otherwise healthy 31-year-old male presented to the emergency department (ED) with one day history of generalized malaise, weakness, subjective fever and chills. He endorsed sub sternal pleuritic chest pain, dyspnea at rest and on exertion. Of note, 2 days prior to symptom onset, he noticed new burning and pruritis on the lateral aspect of his right hip which has progressed into a 10 cm annular rash that was evident on physical examination. On initial presentation, patient was hemodynamically stable. Lab work showed no leukocytosis but was significant for an elevated troponin of 0.76. EKG showed normal sinus rhythm with a right bundle branch block and diffuse ST segment changes with prominent ST segment elevations in inferolateral pattern. CT angiogram of the chest was negative for pulmonary embolism but showed cardiomegaly. Lyme serology was obtained. He denied any tick bite or significant outdoors exposure.His next troponin was elevated at 4.39. He was started on a aspirin, heparin drip, carvedilol and atorvastatin and cardiology was consulted. Patient subsequently had a normal echocardiogram and an equivocal adenosine myocardial perfusion scan. Lyme serology returned negative, however, based on the characteristics of the rash and he was started on empiric Doxycycline. Tick-borne Disease Acute Molecular Panel was sent out and subsequently returned negative. Given concern for myopericarditis a cardiac MRI was obtained and showed evidence of subtle myocarditis in apical inferoseptum with myocardial edema. A diagnosis of Lyme myocarditis was made.The patient clinically improved on carvedilol, atorvastatin, lisinopril and doxycycline and was discharged on a 21-day course of doxycycline. A follow-up Lyme serology 4-weeks later was positive!
Discussion: Usually, Lyme disease occurs in three stages: early localized, early disseminated and late disseminated. However, the stages can overlap and not all patients go through all three. A bulls-eye rash or erythema migrans is usually considered one of the first signs of infection and weeks to months later you can progress to early disseminated stage where you classical have cardiac involvement.(4,6) LC can present as pericarditis, acute myocarditis, endocarditis or pancarditis.(2) Nearly all patients (90%) have atrioventricular block.(5) Myopericarditis is rare and is association with ST segment changes and troponin elevation.(1,2) We believe our patient had presentation was more consistent with myopericarditis based on symptomatology and initial investigations but cardiac MRI showed findings of only myocarditis.
Conclusions: Physicians should be aware that Lyme myocarditis can present early on while serologies may be negative. Antibiotics should be considered early as this is potentially reversible.