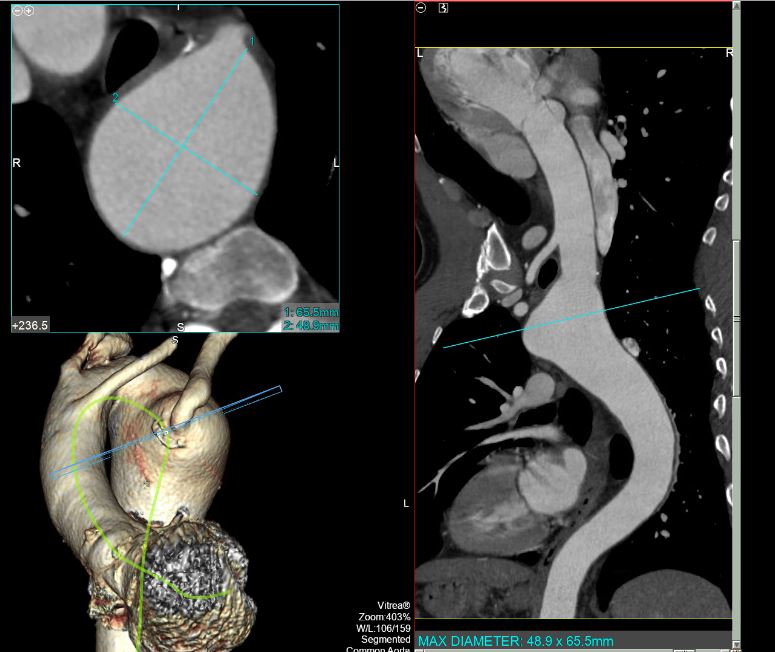
Case Presentation: 56-year-old male patient with PMHx of HTN, HLD, pulmonary embolism and cigarette smoking presented to the emergency department with recurrent chest pain. He described his chest pain as substernal, non-radiating, He was evaluated multiple times for ischemic etiologies of his pain and, associated with SOB but no nausea or vomiting. work up was negative including pharmacological stress test. The patient had multiple similar previous presentations without a clear cause of his chest pain. The patient denies any shortness of breath or dysphagia. During this admission, the patient underwent computed tomography angiogram (CTA) of the chest to rule out aortic dissection, which revealed right sided aortic arch with aberrant origin of the left subclavian artery and an aneurysmal dilatation of the arch measuring 5.5 x 5.1 cm involving the origin of the aberrant left subclavian artery representing Kommerell diverticula. Previous records from outside hospital reviewed and revealed similar findings. It was planned to manage the patient conservatively giving location of the aneurysm and stability in size. The patient underwent a follow up CTA after 6 months with stability in the size of aneurysm.
Discussion: Kommerell diverticula occur in some anomalies of the aortic arch system. It was originally described as a diverticular outpouching at the origin of an aberrant right subclavian artery with a left-sided aortic arch. In severe symptomatic cases, surgical intervention is indicated performing resection of the diverticula and reimplanting the aberrant left subclavian artery into the left common carotid artery to remove any potential substrate for recurrent symptoms of tracheal or esophageal compression.
Conclusions: We are presenting a rare case of a Kommerell diverticula in the setting of an aberrant originating subclavian artery in a right aortic arch. It is originally described in the setting of aberrant right subclavian artery in a left aortic arch. It is important to recognize such cases since Kommerell diverticulum may be asymptomatic or cause symptoms of esophageal or tracheal obstruction. Dysphagia and chest discomfort are common in the adult presentation. Vascular anomalies that do not completely encircle the trachea and esophagus are often asymptomatic and found incidentally. However, they can compress the tracheal bronchial tree and/or esophagus, leading to respiratory or gastrointestinal symptoms.