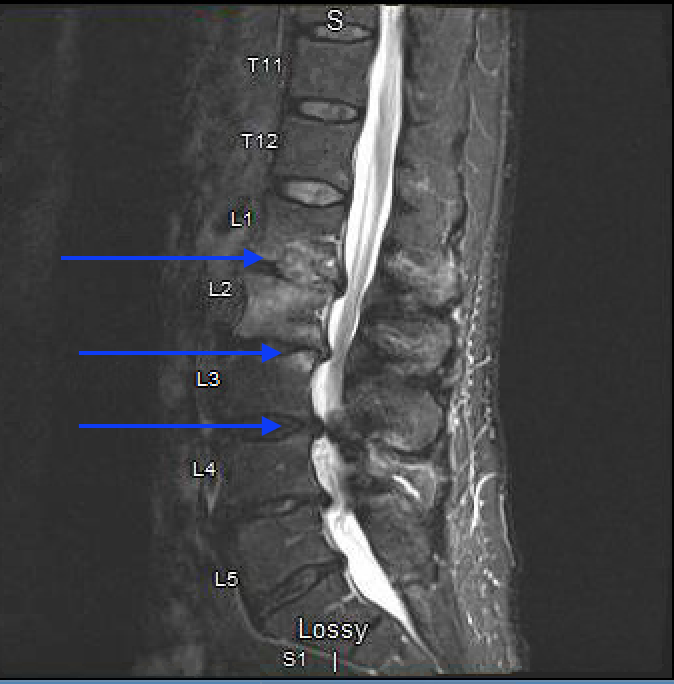
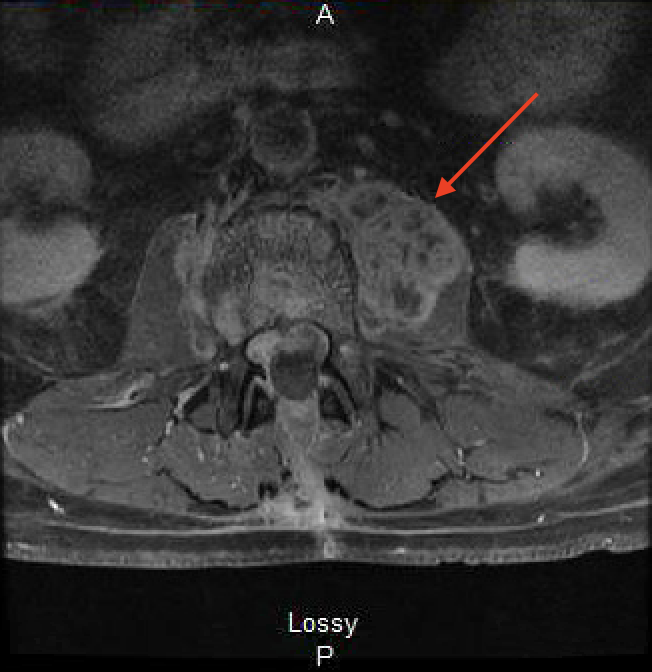
Case Presentation: A 76-year-old man with bladder cancer presented with severe back pain and radiculopathy after receiving treatment with a transurethral resection and subsequent intravesical BCG therapy. His lumbar MRI showed degenerative and morphological changes suggestive of an infection (Figure 1). He was treated with L1-L5 laminectomies and foraminotomies. 3 weeks later, repeat imaging showed worsening and a paraspinal mass. This mass was biopsied and found to be a granulomatous inflammation which had a negative stain for acid fast bacilli, malignancy, or neoplasm. Two weeks later, he returned with additional symptoms including night sweats, fever, and severe pain in the back and right lower extremity. Repeat imaging showed an additional non-enhancing psoas mass (Figure 2). Biopsied lesions showed chronic necrotizing osteomyelitis/discitis and necrotizing granuloma formation. Despite having normal lab values aside from an elevated ESR (72) and CRP (3.3), there was high clinical suspicion for disseminated Mycobacterium Bovis (M. Bovis) infection due to his recent intravesical BCG treatment, so the patient was started on empiric anti-mycobacterial treatment with rifampicin, isoniazid, and ethambutol. He also received vancomycin and cefepime and spinal stabilization surgery was required. M. Bovis was eventually identified as the causal organism via PCR of a prior spinal biopsy specimen.
Discussion: BCG has been a long-standing immunotherapeutic adjuvant to transurethral resection of bladder cancer since 1976, when it was first described to be effective by Lamm et al [1]. While effective, BCG has intrinsic risks. A 2014 review by Asin et al. found a total of 282 reported cases of complications related to BCG immunotherapy between 1975-2013, with 5% of cases resulting in disseminated BCG infection [2]. Vertebral osteomyelitis is a particularly rare presentation of disseminated M. Bovis infection. A recent literature review found 18 cases of BCG induced vertebral osteomyelitis/spondylodiscitis/Pott’s disease making this report the 19th reported incidence in the 40-year history of BCG immunotherapy for bladder cancer [3]. Mycobacterium induced spondylodiscitis is referred to as Pott’s Disease and is responsible for 46% of vertebral osteomyelitis in developing countries [3]. While Pott’s disease is associated with M. tuberculosis, BCG can also be responsible. BCG derived Pott’s disease symptoms can frequently be mistaken for spinal bone metastasis due to this disease being a consequence of bladder cancer therapy [2]. As was seen in our case, the primary spinal involvement is in the thoracolumbar region, namely T6-L5, with secondary symptoms including weight loss and lower extremity radiculopathy subsequent to fever and night sweats [3]. M. Bovis is pyrazinamide resistant so treatment is based on isoniazid, rifampin, and ethambutol with monthly MRI monitoring. Surgical intervention includes decompression, debridement, stabilization, and fusion; it is only indicated for neurological deficits, pathological fractures, or spinal deformities.
Conclusions: Here we present the 19th reported incidence of BCG induced vertebral osteomyelitis/spondylodiscitis/Pott’s disease. While an exceedingly rare complication, M. Bovis Pott’s disease can be a devastating consequence that can be missed by labs that do not reflect the severity of the disease. In these situations, clinical suspicion should drive treatment with early and sustained anti-mycobacterials and surgery if indicated.