Case Presentation: A 48 year-old woman with a history of ulcerative colitis presented to the hospital with a rash and diffuse myalgia of one-week duration. The skin rash was painful and mildly pruritic. She had no fever, abdominal pain, diarrhea, or arthralgia. Physical exam revealed papules on the conjunctivae of her right eye and non-tender, indurated, papulo-nodular plaques with some lesions bearing central necrosis on her scalp, torso, and extremities. Laboratory examination revealed normal white blood cell count, renal, and liver function tests. C-reactive protein and erythrocyte sedimentation rate were 90.9 mg/L and 50 mm/hr, respectively. Anti-nuclear antibody test was negative. Infectious serology including blood culture, HIV 1 and 2 antibodies, fungitell assay, Rickettsia antibodies, and Blastomyces urinary antigen were negative. A swab for bacterial culture and sensitivity from one of the skin lesions was negative. Dermatology was consulted and performed a skin biopsy of a nodule on her right forearm. This revealed a neutrophilic infiltrate without evidence of vasculitis. Histopathologic findings were consistent with acute febrile neutrophilic dermatosis (Sweet’s syndrome). She was started on prednisone 60 mg daily and the appearance of her skin lesions improved. She was discharged home to complete a 14-day prednisone taper.
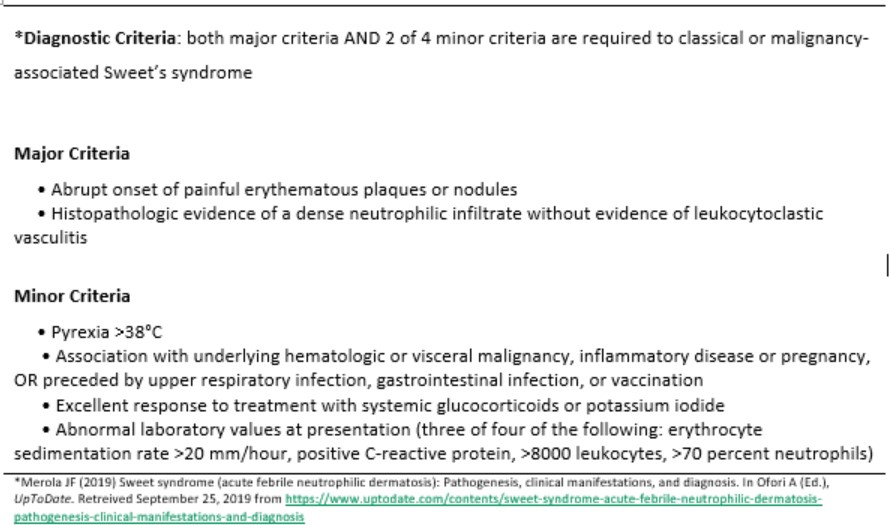
Discussion: While other cutaneous extra-intestinal manifestations of inflammatory bowel disease (IBD) are frequently observed, Sweet’s Syndrome (SS) is rare and seen in less than 1% of patients with IBD (3). Because this dermatosis is usually responsive to treatment, being able to recognize and diagnose SS may dramatically alter a patient’s clinical course. Moreover, SS is associated with malignancy in 20% of cases (4) where many previously undiagnosed patients present with SS as a paraneoplastic syndrome (2). In three-quarter of patients, the rash is accompanied with systemic symptoms such as fever, myalgia, leukocytosis, or GI manifestations of IBD (5). The diagnosis of SS requires the presence of two major criteria and at least 2 of 4 minor criteria. The major criteria include eruption of painful plaques or nodules with the characteristic finding of neutrophilic dermal infiltrate without vasculitis on histopathology (1). Characteristic lesions are painful, erythematous nodules or papules without ulceration that appear on the upper extremities, face, and neck (6). Extra-cutaneous lesions do occur with oral lesions being associated with malignancy (2). Though lesions may recur, treatment with systemic corticosteroids is largely effective.
Conclusions: Hospitalists commonly encounter patients with rash. Sweet’s Syndrome is an uncommon inflammatory disorder that is associated with IBD, malignancy, infections, and drugs. Prompt recognition of SS should lead to an investigation for an underlying disease, when warranted, and initiation of corticosteroid therapy which often results in dramatic improvement of symptoms within days of initiation.