Case Presentation: A 70-year-old male with a past medical history of hypertension presents to the hospital for new onset of right-sided chorea interfering with his everyday activities with no associated weakness, numbness, speech, visual disturbances, rashes, or joint pains. A full initial laboratory work-up was performed notable for non-hemolytic anemia and elevated inflammatory markers. CT head did not show any acute pathology. Magnetic resonance imaging (MRI) of the head revealed ischemic changes to the basal ganglia. EEG showed mild generalized slow activity. CSF analysis showed no evidence of infection or inflammation. The patient was discharged with a neurology follow-up. Huntington’s disease genetic testing was negative. Clinic testing a few months later revealed positive antinuclear antibodies (ANA), double-stranded deoxyribonucleic acid (dsDNA), low C4 complement protein, lupus anticoagulant, anti-cardiolipin, and beta 2- glycoprotein, which fulfilled criteria for the diagnosis of systemic lupus erythematosus (SLE) per American College of Rheumatology (ACR). He was started on oral prednisone (1 mg/kg/day). However, he did not show any signs of recovery. The patient refused any additional immunosuppressive therapy to treat his chorea. Anticoagulation was contraindicated in this patient. Aspirin was prescribed to reduce the future risk of thrombosis.
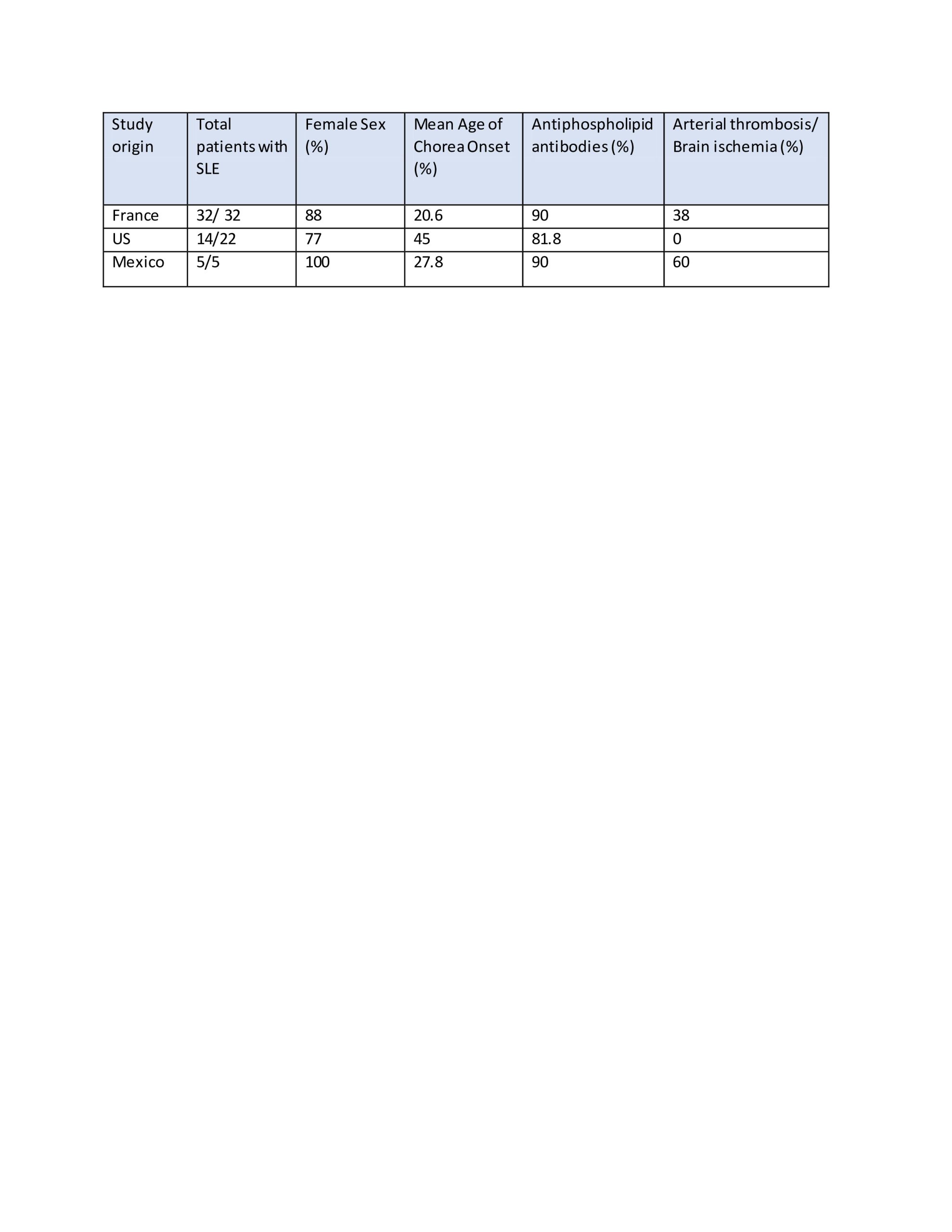
Discussion: The pathogenesis of lupus-associated chorea is still unclear, but it may be related to a vascular, neuronal, and glial injury. Vascular damage may be inflammatory and/or thrombotic [1]. The prevalence of anti-beta 2 glycoprotein I antibodies is higher in SLE patients with the neuropsychiatric disease, it is also present in our patient. This has been mostly described in younger female adults in association with other manifestations of SLE [3,4,5]. Our patient was male, elderly, and had no other features of SLE. Chorea can be the first and at times the only sign prior to the establishment of the diagnosis of SLE. Under such conditions the establishment of the correct diagnosis is difficult, and the chorea may be attributed to a more common etiology [3]. Neuroimaging findings may or may not fit in the clinical picture. Magnetic resonance imaging (MRI) is more sensitive than computed tomography (CT) for neuropsychiatric SLE-associated lesions. Delayed diagnosis and delayed treatment may lead to persistent neurological abnormality as seen in this patient from vascular and/or neuronal damage. EULAR recommendations include steroids with or without immunosuppressive therapy to control disease activity. As seen in prior studies summarized in table-1, the risk of arterial thrombosis is higher in these patients, anticoagulation should be considered if not contraindicated.
Conclusions: SLE with disease onset in old age is rare and is not widely described. Chorea can present as an initial manifestation of SLE. Our report adds to the database a case of lupus associated with chorea with an unfavorable outcome, emphasizing the importance of awareness of this diagnosis and timely treatment.