Background: Hospitals and LTC facilities devote substantial staff time to treating COPD patients requiring intense care. Standard of care (SoC) treatment includes nebulized short-acting beta agonists and muscarinic antagonists (SABA, SAMA, or SABA+SAMA). There is a lack of quantitative data on HCP time dedicated to nebulizations. Workflow mapping confirmed the suitability of T&M methodology to accurately quantify HCP time. The goal of this pilot study was to quantify HCP time and costs associated with nebulized COPD therapy in US inpatient and LTC settings, and to estimate potential efficiencies that could result from newer therapies with less frequent dosing regimens.
Methods: One HCP from each setting completed a survey to describe center characteristics, COPD treatment, and nebulization workflow focused on SABA (albuterol; ALB) and SABA+SAMA (ipratropium bromide and albuterol sulfate; IP/ALB). A Case Report Form (CRF) was built to reflect nebulization workflow. IRB approval for 20 observations was obtained at each site. Staff received training, collected data using stopwatches, and recorded data in the CRF. Time was translated to costs using publicly available salary data and local purchase prices for materials.
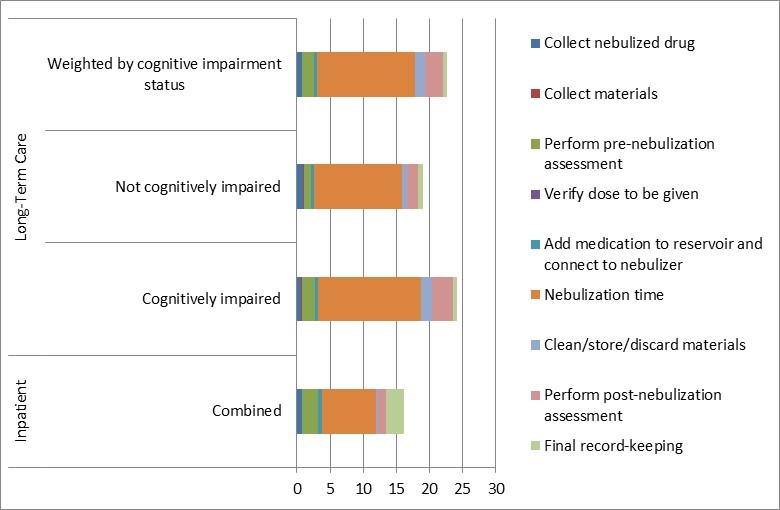
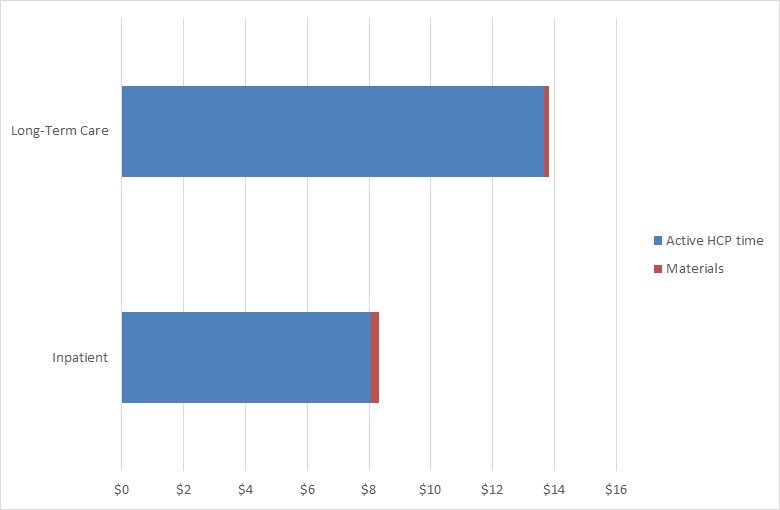
Results: Inpatient observations included 3 ALB and 17 IP/ALB (2 initial and 18 subsequent nebulizations); LTC observations included 5 ALB and 15 IP/ALB (8 patients were cognitively impaired, 12 not). At the inpatient site, all tasks were performed by a respiratory therapist (RT) and at the LTC site by a nurse (RN). Average process time was 16.13 minutes in inpatient (95% CI: 14.48-17.77) and 21.02 minutes in LTC (95% CI: 18.80-23.23), of which 50% and 67% respectively were nebulization time (see Figure 1). At the LTC site, confidence intervals suggest a difference by cognitive impairment status: mean 24.06 minutes (95% CI: 21.29-26.84) if cognitively impaired vs. 18.98 minutes (95% CI: 16.12-21.84) if not impaired. Process time weighted by cognitive impairment status (71% of COPD patients are reportedly impaired and 29% not) is 22.59 minutes.Time/cost modelling compares an estimated frequency of nebulized SoC per day (current dosing) with once-daily dosing. In the inpatient setting, an observed 4.8 nebulizations per day of IP/ALB (weighted by COPD exacerbation severity) and an average LOS of 5.4 days amounts to 7.8 hours of nebulization time per admission. A once-daily nebulized drug would amount to 2.3 hours of nebulization time per admission, a 70% reduction in time. In the LTC setting, current dosing of 2.6 nebulized SoC per day amounts to 32.2 hours of nebulization time per month, while a once-daily nebulized drug would require 13.8 hours, a 57% reduction. In both settings, nebulization materials (one tubing set and one mask/mouthpiece) are stored after nebulization and typically replaced every 9 uses. Applying RT/RN salary data to time spent, average cost of HCP time and materials per nebulization is $8.33 in the inpatient setting and $13.82 in the LTC setting (see Figure 2). Cost modelling in the inpatient setting yields $243 per admission with current dosing versus $72 with once-daily dosing (70% reduction); in the LTC setting, $1,180 per month with current dosing versus $506 with once-daily dosing (57% reduction).
Conclusions: The nebulization process for COPD patients consumes quantifiable HCP time and associated costs. A switch from ALB or IP/ALB to a drug with once-daily nebulization could generate sizable time savings, depending on setting of care and individual site characteristics.