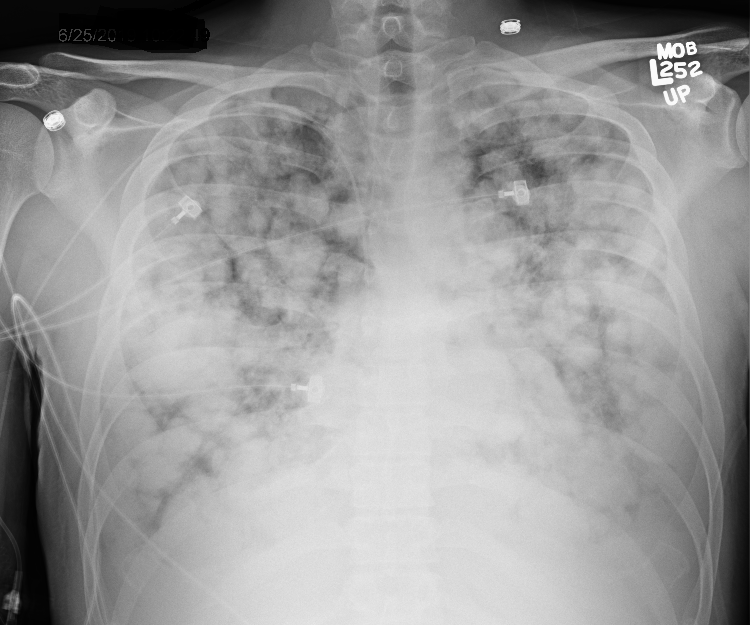
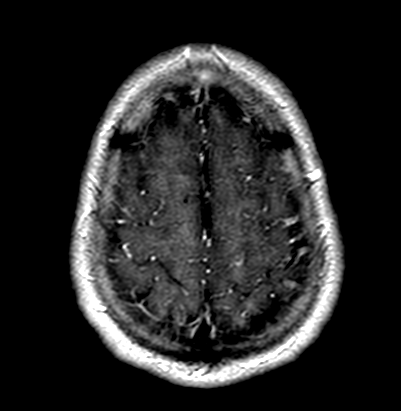
Case Presentation: Patient is a 29 year old male with no significant past medical history who presented for evaluation of worsening shortness of breath and headaches over one month. He had also lost 15 pounds and was experiencing night sweats and significant fatigue. He required ICU admission for hypoxic respiratory failure. CT chest showed multiple pulmonary nodules concerning for metastatic disease. Upon further questioning, the patient endorsed a right testicular mass present for several months, which he believed was a hernia that developed after a sports injury. The mass had been growing rapidly over the past few weeks. Work-up included tumor markers with alpha-fetoprotein (aFP) of 31,274ng/dl, beta-human chorionic gonadotropin (BhCG) <10, and lactate dehydrogenase (LDH) of 500. The patient underwent right orchiectomy and pathology revealed mixed germ cell tumor comprised of 60% yolk sac tumor and 40% teratoma. He underwent staging MRI brain which revealed parenchymal brain lesions. He began therapy with etoposide, ifofamide and cisplatin. Over the course of six months he tolerated treatment well. His brain and lung lesions showed improvement after completion of chemotherapy and his AFP came down markedly to 15.1, but did not normalize. Therefore, monitoring of tumor markers and restaging was done with brain imaging and CT chest, abdomen and pelvis. He was found to have new leptomeningeal disease and a rising AFP. There are plans for him to undergo further chemotherapy, as well as radiation therapy for his brain lesions and possible bone marrow transplant.
Discussion: Although testicular cancer only accounts for 1% of all male cancers, it is the most common solid tumor in men aged 15 to 34. The frequency of brain metastasis is even more uncommon, not exceeding 1.2% of cases and is associated with a poor prognosis. While most testicular germ cell tumors present with a palpable testicular mass, 10% of patients will present with symptoms arising from metastatic disease. Most patients are diagnosed with early stage disease which has a high cure rate. Testicular germ cell tumors are chemosensitive and there can be excellent survival with widespread metastases. The optimal treatment for testicular germ cell tumors with brain metastasis is unknown due to its rarity. For distant metastasis, chemotherapy is typically used as an adjuvant treatment after radical orchiectomy. However, chemotherapy for metastatic brain tumors has poor penetration through the blood brain barrier. Therefore, radiotherapy or surgical intervention can be used as adjunctive therapy to chemotherapy.
Conclusions: Here we report a rare case of non-seminomatous germ cell testicular cancer with metastasis involving the lung and brain. The patient did not present until his metastatic disease yielded symptoms for which he sought treatment. Unlike most cancers, testicular cancer is easily palpable superficially, yet due to its insidious onset and lack of overt signs can go undetected. This case highlights the importance of a thorough physical exam when diagnosing rare conditions.