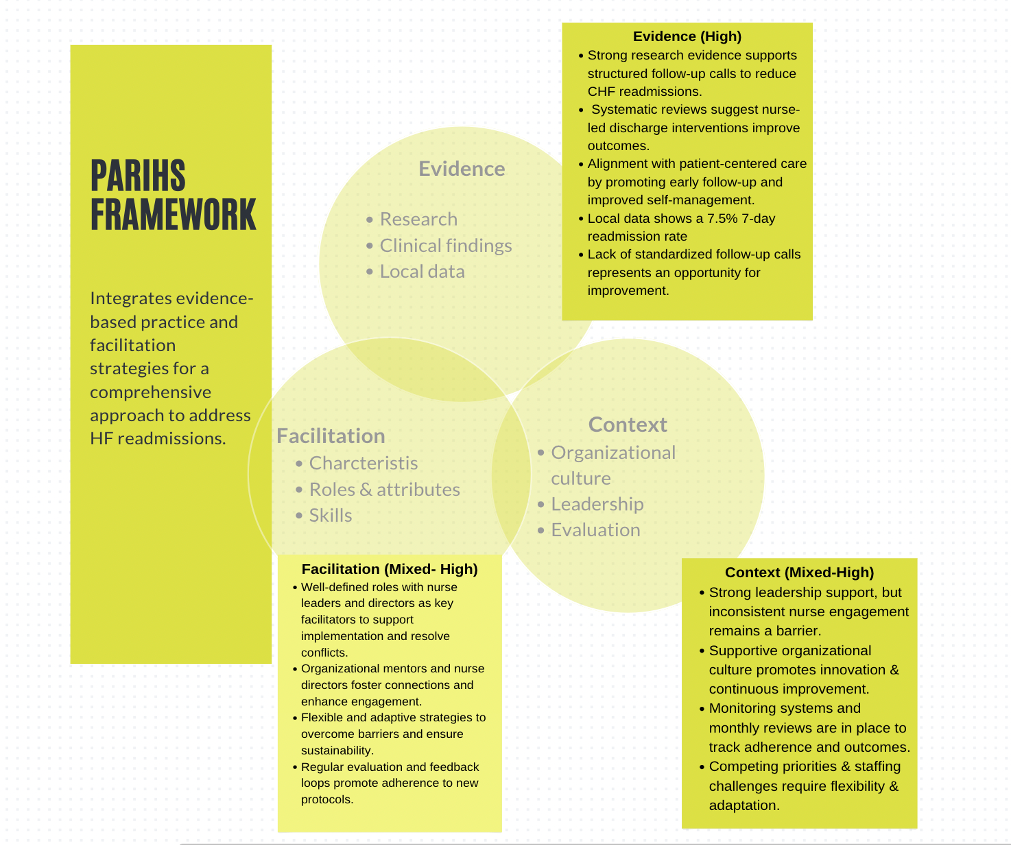
Background: Early heart failure readmissions place a significant burden on hospital resources and worsen patient outcomes,particularly within the first 7 days after discharge. Internal data at a large academic medical center revealed variabilityin transitional care and gaps in timely post-discharge follow-up. Evidence suggests that structured nurse educationand standardized follow-up calls may reduce preventable readmissions. This initiative implemented a targetedtransitional care model aimed at improving continuity of care, enhancing symptom surveillance, and preparing nursingstaff to intervene during high-risk post-discharge periods.
Methods: A pre–post quality improvement design was implemented across two inpatient pilot units. Six nurses responsible fordischarge follow-up received training using evidence-based modules, the AHA Heart Failure Zone-based script, andstandardized telephone protocols. Follow-up calls were conducted within 24–72 hours of discharge and assessedsymptom changes, medication adherence, and escalation needs. Data were collected over six months. Outcomemeasures included 7-day readmission rates, protocol adherence, and nurse knowledge scores using the NKHFEPsurvey. Statistical analyses included chi-square tests, paired t-tests, Spearman’s correlation, and descriptivestatistics. The initiative received IRB designation as a non-research QI.
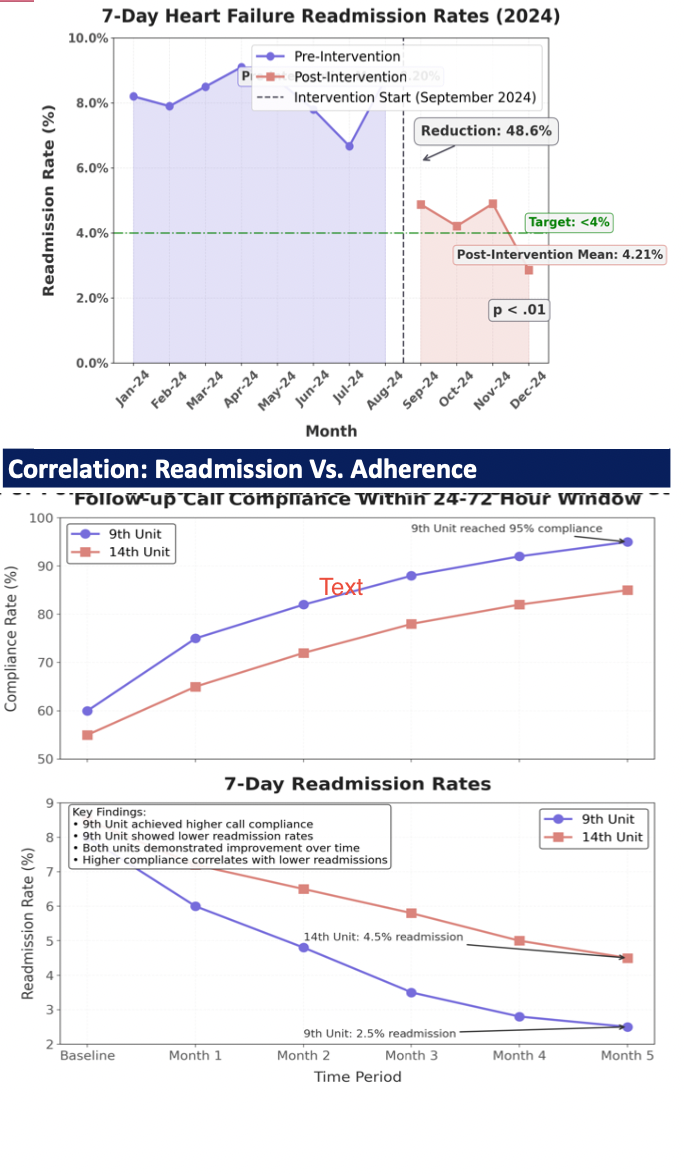
Results: Seven-day HF readmissions declined from 6.28% to 4.21% post-intervention (p = .010). Call adherence reached88.65%, nearing the ≥90% benchmark. Nurse knowledge improved from 62.82% to 89.30% (p < .001). A stronginverse correlation was noted between timely call completion and readmissions (ρ = –0.976, p < .001). Pilot unitperformance varied (χ² = 26.03, p < .001), suggesting workflow integration and leadership engagement influencedimplementation fidelity. These findings support structured follow-up and education as cost-efficient strategies fortransitional care.
Conclusions: Structured post-discharge telephone support and targeted nurse education reduced early HF readmissions andstrengthened transitional care delivery. The intervention was feasible, low cost, and aligned with national qualitybenchmarks. Embedding standardized protocols into existing workflows may offer a scalable strategy to enhancehospital-based care transitions and support management of chronic conditions.