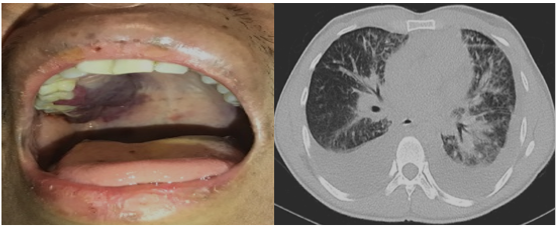
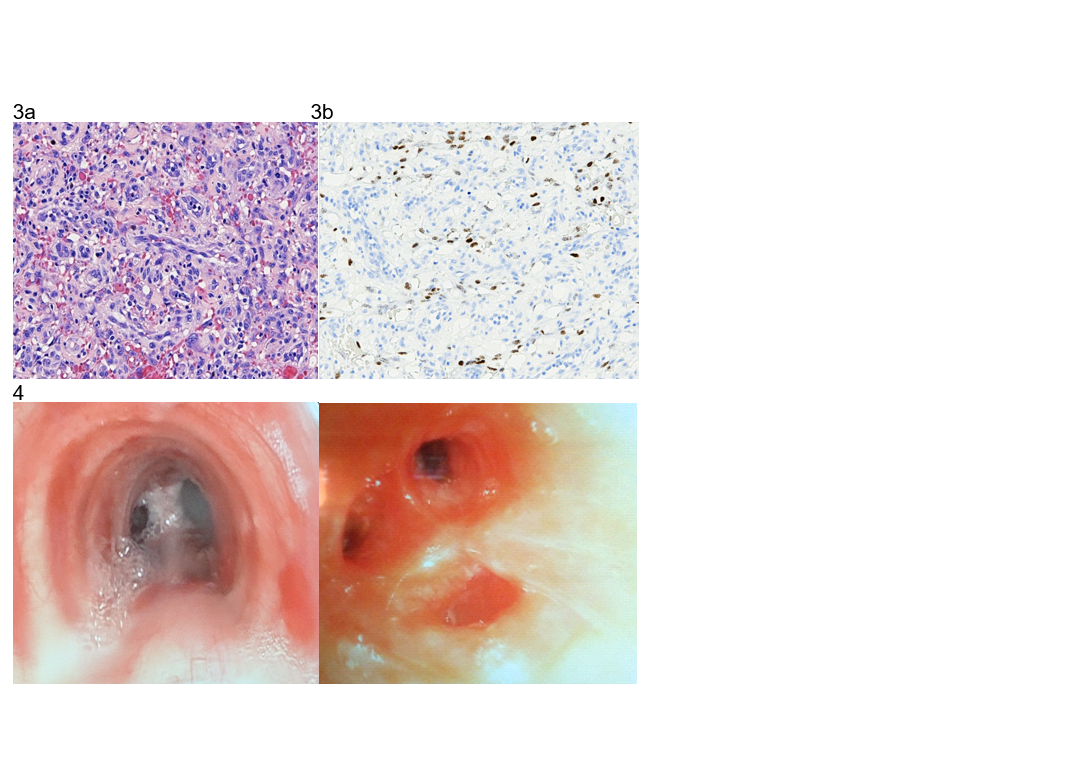
Case Presentation: A 28-year-old male with a recently diagnosed HIV infection presented to the hospital with dyspnea, pleuritic chest pain and fatigue for 4 days. Six weeks prior, he was found to have HIV infection with a CD4+ cell count of 17 cells/ul and an HIV viral load of 41,399 copies/mL. He was prescribed antiretroviral therapy (ART). Physical examination on admission was notable for diffuse skin non-blanching violaceous maculopapular lesions also involving the hard palate. He had a dark red lump on the right eyelid and enlarged non-tender posterior cervical lymph nodes; lung exam identified bilateral crackles.Testing revealed thrombocytopenia, a CD4+ T-lymphocyte count of 64 cells/ul with an HIV viral load of <20 copies/mL. A chest CT scan showed large bilateral pleural effusions and multifocal airspace opacities.A thoracentesis showed a pleural fluid with 160 white blood cells and 105,300 red blood cells. A biopsy of one of the skin lesions was characteristic of Kaposi’s Sarcoma (KS). Bronchoscopy revealed multiple violaceous raised lesions throughout the bronchial airways, visually consistent with disseminated KS. A transthoracic echocardiogram revealed early signs of cardiac tamponade. Bartonella serology was negative. Biopsies of the palate and the eyelid mass also showed findings compatible with KS.Due to the extent of disease and persistent symptoms, Doxorubicin based chemotherapy was initiated.
Discussion: Kaposi’s sarcoma is one of the most common cancers in patients with AIDS, i.e. with HIV infection and CD4+ cells under 200 cells/uL. The incidence of KS in the United States peaked at 47 cases per million people per year in the early 1990s. With the advent of highly active ART and improved immune reconstitution, KS now occurs at an incidence rate of about 6 per million each year. Cutaneous KS presents as violaceous lesions on skin and mucosal surfaces. In individuals with advanced immunodeficiency, the presence of skin lesions raises the possibility of concomitant visceral involvement. Pulmonary manifestations of KS include characteristic airway lesions, peribronchovascular opacities, and hemorrhagic pleural effusions. Pericardial effusions can develop and can cause hemopericardium. KS generally involves epithelial cells on the serosal surfaces rather than free flowing cells in the reactive effusions, therefore cytologic analysis of pleural and pericardial fluid does not generally reveal findings diagnostic of KS. Cutaneous KS may resolve with ART-induced immune reconstitution alone. In cases of visceral involvement, Doxorubicin-based chemotherapy along with ART is generally recommended. The major goals of therapy of KS are preventing the progression of the disease by reducing the tumor burden thereby reducing organ compromise. After six sessions of chemotherapy, and on ART, our patient showed clinical improvement. His skin lesions regressed, his respiratory symptoms resolved.
Conclusions: KS and its complications are encountered less frequently with the decreased prevalence of advanced AIDS due to improved ART. However, in situations where patients present with, or otherwise develop, advanced AIDS, KS may still occur and may be a presenting manifestation. Recognizing KS lesions and considering KS in differential diagnoses remain important clinical skills. As patients with visceral KS are likely to present with finding which prompt hospitalization, Hospital Medicine plays an integral role in ensuring proper recognition, management and coordination of care for such patients.