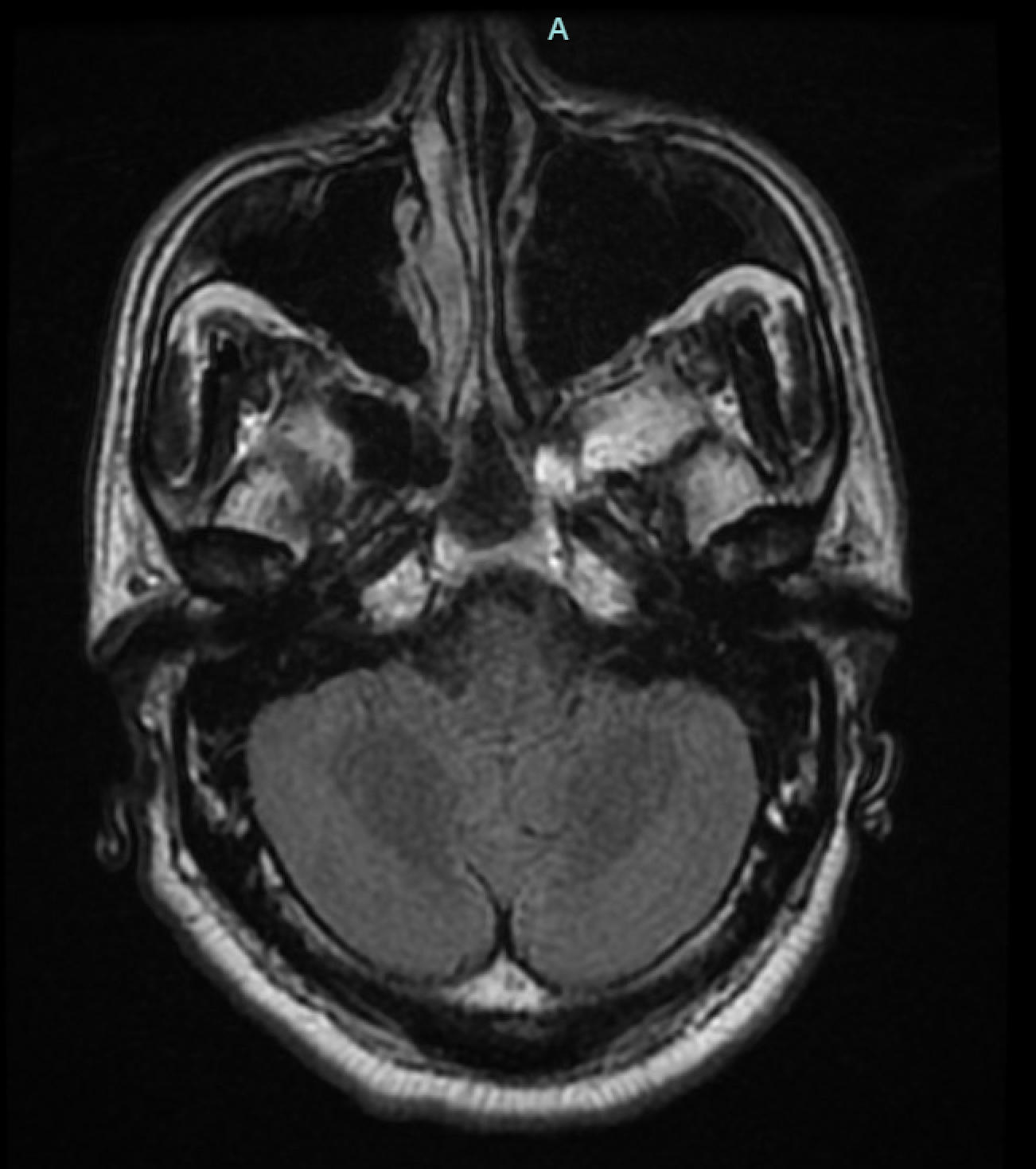
Case Presentation: A 51year old male with a past medical history of hyperlipidemia, anemia, tobacco abuse, and mild intermittent asthma who presented for evaluation of altered mental status. History was obtained from patient’s wife and brother who were present at the bedside as patient was intubated. Per family, patient reported having a headache 2 days prior that improved and body aches yesterday. Denied any other symptoms besides body aches. Took Nyquil last night but wife reports that upon waking this morning, he was not in bed. She found him on the couch, difficult to arouse, and not appropriately speaking, prompting wife to call 911. Denies any recent travel but reports daughter has a cold currently. Reports that the patient does not use any drugs or drink alcohol routinely. Of note brother was concerned wife was poisoning him. In the ED, patient was intubated for airway protection. Patient was hemodynamically stable. Labs not significant. Urine drug screen and blood alcohol level were negative. CT head and CXR negative. He underwent lumbar puncture (LP) and it came back positive for Varicella-Zoster Virus (VZV). Patient was treated Ampicillin and Vancomycin but stopped after LP came back positive for VZV and continued on IV Acyclovir and Ceftriaxone, the later for sinusitis noted on MRI brain completed later. Patient was eventually extubated and was noted to be back to baseline per wife at bedside. He was discharged home in stable condition. Of note our patient denied any history of chickenpox as a child.
Discussion: VZV is a double strand, unique human DNA virus with high affinity for skin, mucous membrane, and nerve tissue. It can be transmitted to human beings through respiratory tract, skin, and mucous membrane. The first infection usually occurs in children and causes chickenpox which is mainly manifested as herpes zoster distributed along the peripheral nerve, then the virus lurks in the peripheral ganglion, cerebral ganglion, the posterior root ganglion of spinal cord, and autonomic ganglion along the nerve axis. Under the circumstance of fatigue, cold, and decreased body immunity, the virus revives to cause reinfection. The reactivated VZV invades the ectodermal tissue and reaches the innervated area along the nerve axons that cause a variety of nervous system damage in peripheral and central nervous system. The main manifestations are herpetic neuralgia, cranial neuropathy, meningitis, meningoencephalitis, encephalitis, and even myelopathy and cerebrovascular disease. Among them, meningitis and meningoencephalitis are the most common complications of VZV central nervous system infection. This is an interesting case because collateral history from family made it seems as though patient was poisoned by unknown drug/substance. However, he was eventually diagnosed with VZV encephalitis. Patient presented during the late spring months in May. According to previous reports, there was a debate about whether the incidence of herpes zoster is seasonal. Some studies have found that VZV meningitis is more likely to occur in winter, but VZV encephalitis in general does not have a consistent or strong seasonal variation.
Conclusions: When a patient presents with altered mental status it is important to obtain a good history, perform physical and neurological exam but meningitis/encephalitis should always be considered in the differential. If there is high suspicion a LP should be performed to rule meningitis/encephalitis in or out.