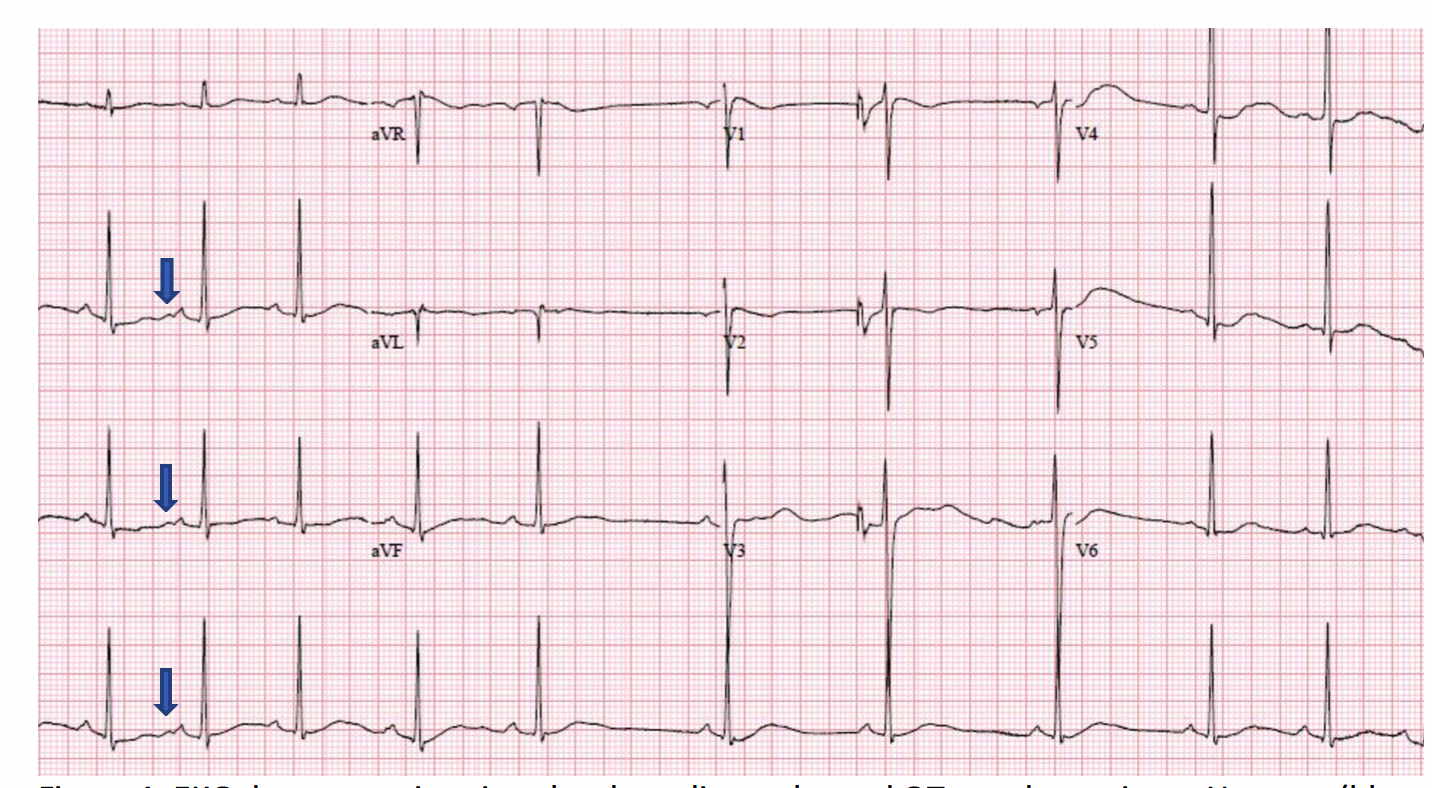
Case Presentation: A 15 year old man presented with two hours of inability to move his extremities. The night prior, the patient had been playing football without protective padding. He experienced a hit to his back resulting in a fall, and noted that he developed bilateral thigh tingling approximately one hour after this. This progressed over the course of the night to gait instability, at which time he presented to a local emergency department. He underwent an MRI of his thoracic and lumbar spine, which was normal. The patient reported that his symptoms gradually improved without intervention, and he was discharged to home. The patient was able to ambulate when leaving the emergency room, but still reported sensation of tingling in his thighs. When the patient awoke the following morning, he was unable to get out of bed. He described a sensation of not being able to move his arms or legs at all, as well as diaphoresis and overall feeling poorly. On presentation, the patient was noted to have a heart rate of thirty-five beats per minute. He had one out of five strength in his left upper extremity and bilateral lower extremities, and three out of five strength in his right upper extremity. Sensation was intact throughout. Speech was intact, and pupils were equal, round and reactive. An EKG demonstrated sinus bradycardia, U waves, and a prolonged QTc. Potassium was 1.5 mEq/L. The remainder of the basic chemistry panel was within normal range, including renal function, sodium, chloride, and bicarbonate. Urine potassium was elevated. Serum renin and aldosterone levels were normal. Urine toxicology was negative for illicit drugs. The patient’s potassium was repleted over the course of the next twelve hours. As the potassium was repleted, the patient had complete resolution of his muscle weakness. His bradycardia, diaphoresis, and sensation of feeling poorly resolved. Genetic testing was obtained and ultimately demonstrated a heterozygous pathogenic mutation in the skeletal muscle sodium channel, SCN4A, consistent with hypokalemic periodic paralysis.
Discussion: Hypokalemia is common problem encountered by hospitalists, and it is important for providers to recognize the neuromuscular and cardiovascular manifestations. While not a common condition, hypokalemic periodic paralysis should be considered in a patient presenting with profound hypokalemia. Hypokalemic periodic paralysis is a neuromuscular disorder related to abnormal muscle calcium or sodium channels. In patients with this disorder, periods of heavy exertion, fasting, or high carbohydrate meals can result in an abnormal influx of potassium intracellularly, causing profound muscle weakness and hypokalemia. Hypokalemic period paralysis is typically inherited in an autosomal dominant fashion with incomplete penetrance. Patients with hypokalemic periodic paralysis typically present in childhood or adolescence with periodic attacks of weakness, without loss of consciousness, respiratory difficulty, or bulbar symptoms.
Conclusions: Our patient was discharged after normalization of potassium and resolution of symptoms. He was given a prescription for potassium pills as needed to take at the onset of episodes of muscle weakness. When seen in follow up, the patient was feeling well and resumed normal activities. The majority of patients with hypokalemic period paralysis will go on to develop a myopathy later in life, typically manifesting after age 50. The severity of this myopathy is variable, and it is unclear if severity is related to the number of paralytic attacks.