Background: Large volume paracentesis is commonly performed in patients with refractory ascites but can induce hypotension and kidney injury. There is evidence that administering albumin at 6-8 grams per liter (g/L) of ascites removed during or after paracentesis can reduce these adverse events. Current guidelines recommend this practice when >2 liters are removed in high-risk patients or >5 liters are removed in any patient. Despite these guidelines, clinical practice still varies widely. We retrospectively analyzed the association of albumin dosage and adverse events following large volume paracentesis in hospitalized patients at a single academic teaching hospital.
Methods: Patient and procedural data were obtained from a registry of all procedures performed by a hospitalist procedure service at a single academic teaching hospital from June 2013 to July 2018. We identified all patients who underwent large volume paracentesis (>2 L) and obtained electronic health record data on vital signs, laboratory tests, patient demographics, severity of illness, and albumin administration. We excluded patients with severe chronic kidney disease (CKD) (baseline serum creatinine [Cr] >3), who lacked a peri-procedural Cr, for whom peri-paracentesis albumin was not indicated, or who received >35 g/L of albumin (as this was considered treatment dosing for hepatorenal syndrome). Albumin administration was categorized as 6-8 g/L vs. >8g/L. We used multivariable logistic regression to test the association between dose of albumin administered and the primary outcome, acute kidney injury (AKI), defined as >30% increase in post-procedure serum creatinine within 72 hours. We also used multivariate linear regression to examine a secondary outcome of mean change in systolic blood pressure (SBP) over 24hrs post-procedure.
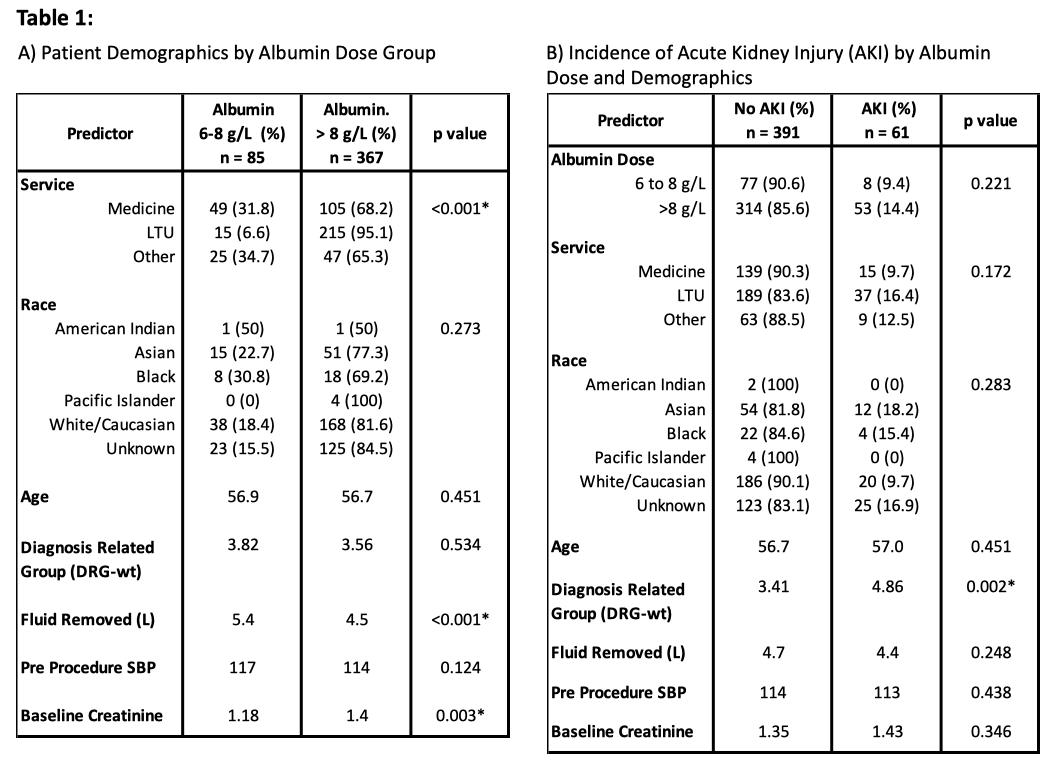
Results: A total of 452 patients without baseline severe CKD underwent >2L paracentesis and were eligible for analysis, of whom 182 had >5L removed. One hundred fifty-four (34%) were on the general medicine service, 226 (50%) on the liver transplant service, and 72 (16%) on all other services. In all, 85 (19%) patients received 6-8 g/L, and 367 (81%) received >8 g/L of peri-procedural albumin. Patients who received >8 g/L of albumin were more likely to be on the liver transplant service or have a higher baseline Cr (Table 1). Multivariate analysis showed that albumin dose was not associated with post-procedure AKI (10.4% in 6-8 g/L vs. 16.9% in >8 g/L, adjusted odds ratio 1.35 [95% CI: 0.57-3.23], p=0.497). Post-paracentesis mean change in SBP also did not significantly differ by albumin group (mean SBP drop of 2.95 in 6-8 g/L vs. 4.36 in >8 g/L, R= 1.31 [-1.24 – 3.86], p=0.312).
Conclusions: Patients undergoing large volume paracentesis at our institution received widely varying doses of peri-procedural albumin, with the majority of patients receiving >8 g/L. Albumin doses higher than current guidelines were not associated with a lower incidence of AKI or mean drop in SBP following paracentesis. Given the high cost of albumin and potential for worsening volume overload, guideline-recommended dosing should be more consistently adopted.