Background: Timely post-discharge office visits reduce readmission risk, but the association between telemedicine follow-up visits and readmission in patients discharged from the medicine service remains unclear. The COVID-19 pandemic led to a significant increase in telemedicine utilization for post-discharge follow-up, prompting questions about its association with readmission. Thus, our primary objective was to assess the association between post-discharge telemedicine follow-up and 30-day readmission, compared with in-person office visits.
Methods: This is a retrospective, multicenter cohort study of 99,479 adult patients discharged from the Medicine Service in an integrated healthcare system, before (January 1, 2017 – February 29, 2020) and during (March 1, 2020 – December 31, 2021) the COVID-19 pandemic. Patients were excluded if they were discharged to hospice or skilled nursing facilities; transferred to another hospital; died during hospitalization; or died prior to follow-up visit completion. Patients admitted for COVID-19 were excluded due to specialized post-discharge follow-up protocols. The exposure was telemedicine (telephone or video) versus in-person office visit within 7 days post-discharge. When assessing risk of 30-day readmission (primary outcome) and 30-day ED visits (secondary outcome), inverse probability of treatment weighting (IPTW) and competing risk analyses were used to account for the competing event of mortality and adjust for confounding. Cox proportional hazards modeling with IPTW was used to assess the risk of all-cause 30-day mortality (secondary outcome). Adjusted hazard ratios (aHR) and 95% confidence intervals (CI) were reported for outcomes. Demographic and clinical variables in the regression analyses included age, sex, race/ethnicity, body mass index, comorbidity index and acute illness severity scores, length of stay, and any surgery during hospitalization; variables most proximate to discharge included vital signs, hemoglobin, sodium, creatinine, and use of supplemental oxygen. All statistical analyses were performed using SAS software version 9.4 with the threshold of significance set at two-sided p< 0.05.
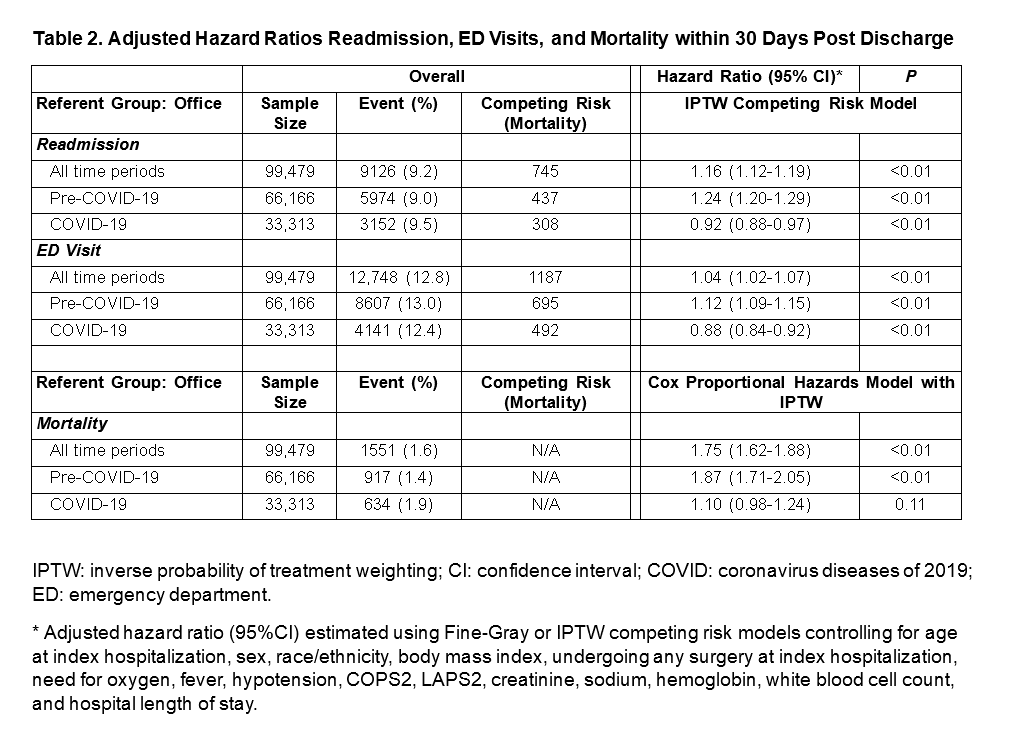
Results: Among 99,479 patients discharged from the Medicine Service, 49.9% (49,687) received telemedicine follow-up within 7 days post-discharge. The mean age was 67.2 (SD 16.4) years, and 48.9% were female. Pre-COVID-19, 28.2% of patients received telemedicine follow-up, which was associated with a higher 30-day readmission risk compared to in-person office visits (aHR 1.24, 95% CI: 1.20–1.29, p< 0.001). During the COVID-19 pandemic, telemedicine comprised 93.2% of follow-up visits and was associated with decreased readmission risk (aHR 0.92, 95% CI: 0.88–0.97, p< 0.001). Additionally, telemedicine was associated with a lower risk of ED visits (aHR 0.88, 95% CI: 0.84–0.92, p< 0.001) and no significant difference in mortality (aHR 1.10, 95% CI: 0.98–1.24, p=0.11) compared to in-person visits during the pandemic.
Conclusions: Post-discharge telemedicine visits during the COVID-19 pandemic were not associated with higher readmission risk compared to in-person visits and were, in fact, associated with a lower risk of readmission. Differences in readmission risk observed prior to the pandemic may have been due to patient selection. These findings highlight telemedicine as a safe and effective alternative to in-person follow-up care, supporting its integration into a flexible, hybrid model for discharge planning.