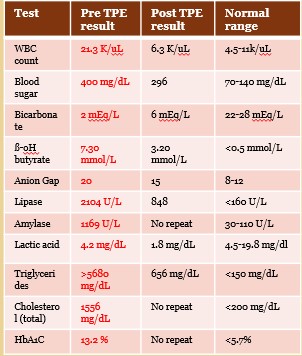
Case Presentation: A 21-year-old female (assigned male at birth) presented with 5 days of worsening nausea, vomiting, and abdominal pain. She had a known history of type 1 & 2 diabetes mellitus, obesity, psoriasis, and major depression. On estradiol for gender-affirming therapy for the past year. Over the last 6 months, had 4 episodes of acute pancreatitis complicated by diabetic ketoacidosis (DKA). These episodes were attributed to medication and insulin non-adherence. During this episode, she was brought in from outside hospital with aforementioned symptoms. Her presenting labs and CT Scan consistent with acute pancreatitis and DKA. On checking lipid panel, was found to have an alarmingly high triglyceride (TG) level of 5680 mg/dl. Patient admitted to the medical ICU and started on fluids, insulin drip, pain management, and antiemetics. Fenofibrate was begun in an attempt to lower triglyceride levels, and estrogen replacement therapy was held. Given concomitant acute kidney injury, nephrology was consulted. Therapeutic plasmapheresis was initiated, which reduced TG level to 656 mg/dl. Over the next few days, her symptoms gradually improved, and repeat CT scan showed necrosis of pancreatic head and neck with multiple necrotic pseudocysts. Discharged on fenofibrate and atorvastatin with outpatient gastroenterology and endocrinology follow up. Unfortunately, due to socioeconomic conditions, follow-up was difficult. Patient restarted hormonal gender-affirming care shortly afterwards. Has had multiple similar episodes since.
Discussion: Transgender individuals on gender-affirming care often require higher doses of hormonal therapy for extended durations of time. While cardiovascular effects of estrogen therapy are well described, there is more awareness regarding estrogen being responsible for marked elevation in TGs (1), particularly in those undergoing gender-affirming care with hormone therapy, those with familial predisposition, and those with poorly controlled diabetes. Hypertriglyceridemia causes acute pancreatitis in turn by increasing blood viscosity and ischemia of the pancreatic capillary bed. Further, increased free fatty acids from TG cleavage are toxic to pancreatic acinar and endothelial cells. Acute pancreatitis is a stressful, life-threatening situation that could in turn trigger DKA. Per the 2023 American Society of Apheresis, plasmapheresis is a category 3 recommendation in treating hypertriglyceridemia-induced acute pancreatitis (2). The 2021 French Society of Anesthesia and Critical Care recommends initiation of plasmapheresis if medical therapy proves to be insufficient (3). However, it is still unclear if plasmapheresis is superior to conventional therapy with insulin drip in terms of mortality, time to organ failure resolution, and ICU/hospital length of stay (4,5).
Conclusions: Hormonal gender-affirming care with estrogen could potentially be a risk factor in causing severe hypertriglyceridemia resulting in recurrent bouts of acute pancreatitis that can be life-threatening. Risk factor is elevated in those with diabetes mellitus and those with a familial predisposition. Therefore, screening patients with serial lipid levels is crucial to uncover those who are predisposed to hypertriglyceridemia. Therapeutic plasma exchange can help in early and effective reduction of TG levels. However, so far, no clear evidence that it is better than intensive insulin therapy. Need to identify subgroups in whom it may be more effective