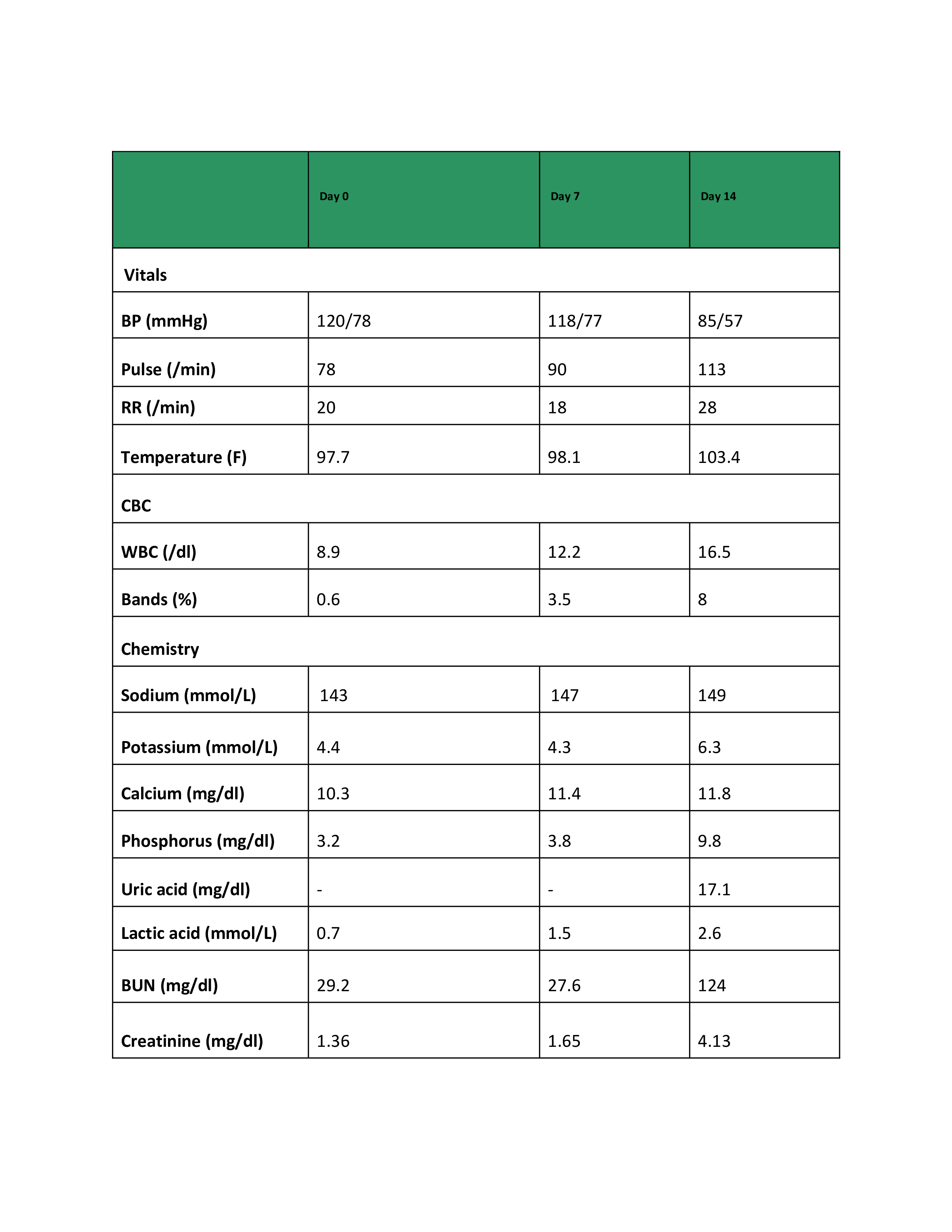
Case Presentation: 91-year-old Caucasian male with dementia, prostatic adenocarcinoma, and chronic urinary retention with an indwelling foley catheter. He was found unresponsive after an unwitnessed fall at his assisted living facility. His family noted progressive cognitive decline with hallucinations over the prior month and a 2-week history of erythematous maculopapular rash on the chest. On admission, creatinine was 1.36 mg/dl, urinalysis suggested catheter-associated Urinary Tract Infection (CAUTI). Imaging further showed no acute intracranial abnormality, mild interstitial edema with small pleural effusion, and mild right hydronephrosis. He was diagnosed with acute metabolic encephalopathy from CAUTI and treated with broad spectrum antibiotics. During hospitalization, the rash progressed rapidly with clinical deterioration (table) and severe sepsis. Sweet syndrome was suspected and punch biopsy performed. Blood and urine cultures remained negative. He developed treatment-resistant, PTH-independent hypercalcemia, concerning for malignancy. Skin biopsy revealed dermal infiltration by atypical B-cell, high proliferative index (Ki-67>90%). IHC was positive for CD20, CD10, c-Myc, and BCL-2. FISH identified c-MYC and BCL2 rearrangements, negative for BCL-6, MUM1, HHV8, and EBV, confirming High-Grade B-cell Lymphoma (HGBL) with MYC and BCL2 rearrangements, consistent with double-hit lymphoma with primary cutaneous involvement. Despite escalation of care, his clinical course was fulminant, and he succumbed within two weeks of admission.
Discussion: Although HGBL with MYC and BCL2 rearrangements account for only ~1–2% of non-Hodgkin lymphomas, they behave aggressively and require timely recognition. Cutaneous manifestations are rare in systemic HGBL and often mimic benign or inflammatory conditions. Indeed, a review of secondary cutaneous lymphomas emphasises that skin dissemination from systemic lymphoma is frequently under‐recognised and carries a poor prognosis (5-year survival ~30 % vs 87 % for primary cutaneous forms). For hospitalists, the critical learning point is that rapidly progressive skin lesions in the setting of systemic instability should prompt early skin biopsy. Early biopsy enables immunophenotyping and FISH testing — required for diagnosing double-hit lymphoma and differentiating systemic secondary cutaneous involvement from primary cutaneous lymphomas, such as mycosis fungoides, Sézary syndrome, or indolent cutaneous B-cell lymphomas, which carry a dramatically different prognosis and management strategy. Furthermore, delayed tissue diagnosis is associated with missed opportunities for timely systemic therapy. Hospitalists play a pivotal role, as they are often the first to encounter these skin findings during acute decline. Education and awareness are essential so that bedside assessment incorporates dermatologic evaluation, early biopsy, and multidisciplinary coordination with dermatology and hematology.
Conclusions: This case highlights the importance of maintaining vigilance for hematologic malignancy in patients with unexplained, rapidly evolving cutaneous lesions and systemic deterioration. Early skin biopsy is central to timely diagnosis, risk stratification, and initiation of appropriate therapy. Targeted education for hospitalists and frontline inpatient providers can reduce diagnostic delay and improve outcomes in patients with aggressive lymphomas presenting with atypical cutaneous findings.