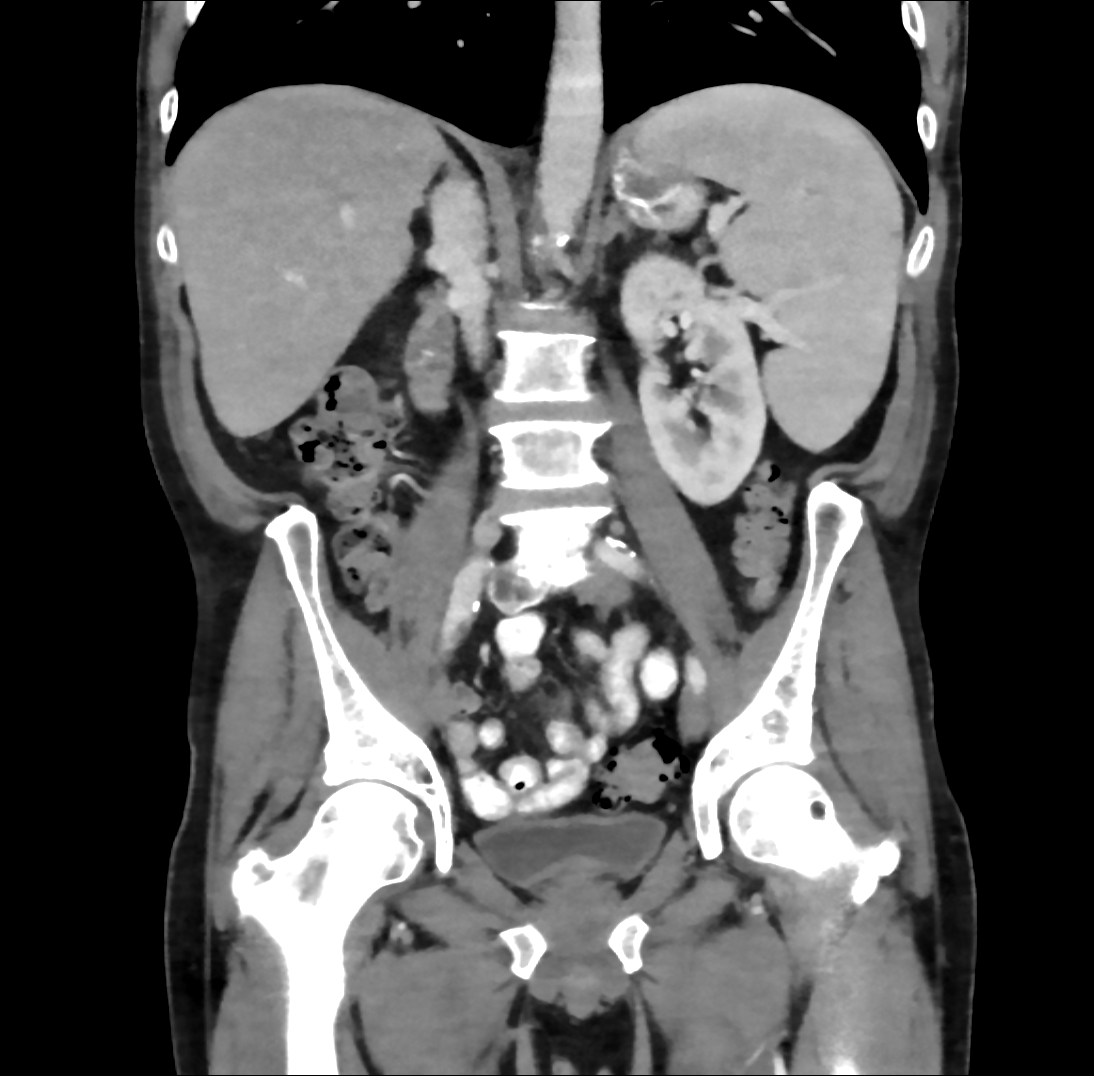
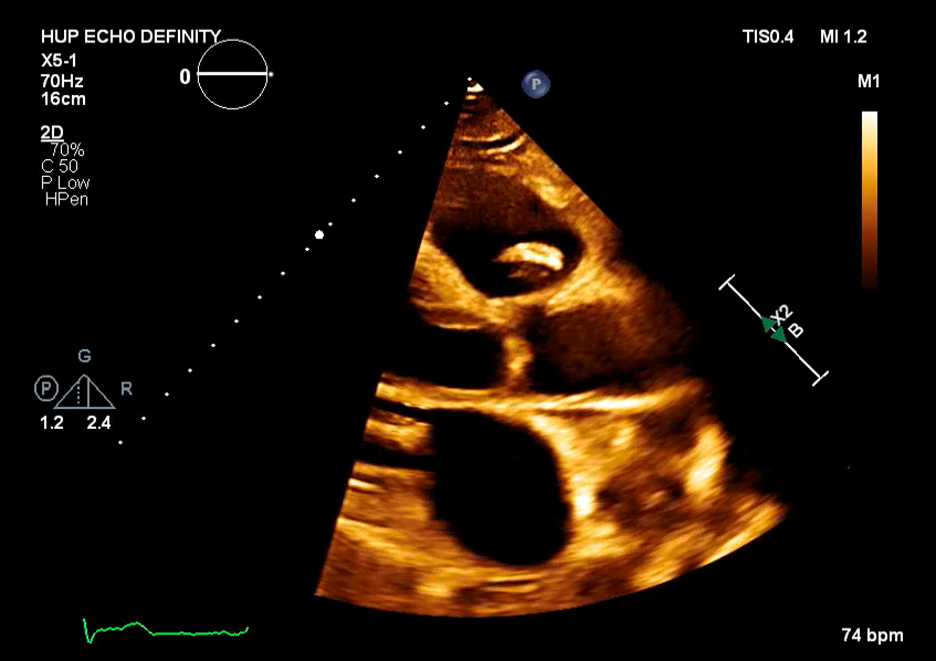
Case Presentation: 61-year-old man with coronary artery disease, tobacco use, and partial R toe amputation after trauma presented to an outside hospital with 3 months of fevers, night sweats, and 30 kg weight loss. He was found to have pancytopenia, splenomegaly, and retroperitoneal lymphadenopathy raising concern for malignancy. These findings prompted a bone marrow biopsy which showed trilineage hyperplasia without evidence of hematological or metastatic neoplasm. Extensive coronary calcifications were incidentally noted on imaging. He was discharged with plan for Hematology and Cardiology follow-up. He presented to our hospital with persistent symptoms. On exam, he was febrile to 39.2C, tachycardic, and had a 3/6 holosystolic murmur at the apex. Labs showed pancytopenia with WBC 4.5, hemoglobin 8, and platelets 47K. Blood cultures were obtained and vancomycin, cefepime, and azithromycin were administered. In less than 24 hours, blood cultures returned positive for streptococcus parasanguinis and antibiotics were narrowed to ceftriaxone. Transthoracic and transesophageal echocardiograms demonstrated a large (1.4 x 0.6 cm) pulmonic valve vegetation with severe pulmonic valve regurgitation and ruptured posterior mitral valve leaflet chordae with severe mitral valve regurgitation. The size of the vegetations and degree of valvular dysfunction prompted urgent surgical consultation and he subsequently underwent pulmonic and mitral valve replacement with concurrent coronary artery bypass grafting for high grade right coronary artery stenosis. Intraoperative exam demonstrated large pulmonic valve vegetations and bi-leaflet mitral valve vegetations. Withing 72 hours of antibiotic initiation, he reported clinical improvement with resolution of fevers and night sweats and improvement in his appetite and energy level and subsequently completed a 6-week course of ceftriaxone. Interestingly, during his admission to our hospital, his prior bone marrow biopsy was reviewed and found to be suggestive of low-grade myelodysplastic syndrome (MDS). On most recent laboratory testing, obtained at completion of antibiotics, he remains mildly pancytopenic.
Discussion: Infectious endocarditis (IE) is a clinical entity with high mortality rate even with antibiotics and/or surgery. Concomitant left and right sided endocarditis accounts for 13% of all IE cases. (1,2) Risk factors for right sided endocarditis include intravenous drug use, implanted cardiac devices, immunosuppression, and presence of an underlying right-sided cardiac anomaly. Presenting symptoms of IE can often be nonspecific including fever, malaise, weight loss, night sweats, as well as symptoms secondary to septic emboli if. Physical exam findings of Janeway lesions, Osler nodes, and splinter hemorrhages, often heralded as stigmata of IE, are present in only 3-5% of patients. (3) More notably, splenomegaly (thought to be due to immune stimulation due to IE) is present in 10% of patients. (4) In this patient, his constitutional symptoms combined with pancytopenia, lymphadenopathy, and splenomegaly, raised concern for malignancy and biased his diagnostic workup leading to a delay in diagnosis. Interestingly, the possibility of low-grade MDS may have contributed to the patient’s presentation or alternatively may be secondary to chronic infection.
Conclusions: In a patient presenting with nonspecific B symptoms and splenomegaly, it is important to also evaluate for indolent infections in addition to appropriate malignancy work-up.