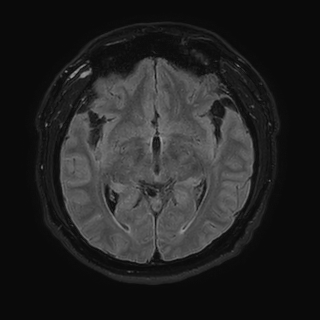
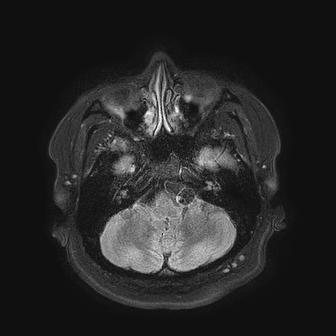
Case Presentation: A 30-year-old man presented with five days of progressive holocephalic headache, posterior neck pain, and photophobia. He denied fever, focal weakness, sensory disturbances, or recent trauma. He emigrated from rural Guatemala ten years prior. Meningeal signs were present, including nuchal rigidity and pain with neck flexion, but his exam was otherwise normal. Non-contrast CT head showed prominent CSF-density spaces at the vertex, a finding that can mimic atrophy but is atypical for a patient of this age. Lumbar puncture demonstrated 42,000 red blood cells with otherwise unremarkable indices. MRI of the brain with and without contrast revealed diffuse fluid-attenuated inversion recovery (FLAIR) hyperintensity and corresponding susceptibility-weighted imaging (SWI) hypointensity throughout the sulci. These findings were interpreted as concerning for subarachnoid hemorrhage. However, CT angiography of the head and neck was unremarkable without evidence of aneurysm, arteriovenous malformation, or vasculitis. Repeat MRI after 48 hours demonstrated interval resolution of the diffuse sulcal FLAIR hyperintensity and SWI hypointensity, and revealed multiple well-circumscribed CSF-isointense subarachnoid structures, with focal prominence and adjacent mass effect, suggestive of space-occupying cystic lesions. One cyst along the left sylvian fissure contained a small T2-hyperintense eccentric nodule consistent with a scolex. Given the imaging findings and epidemiologic risk factors, CSF was sent for Taenia solium polymerase chain reaction (PCR) and cysticercus antigen testing. Both tests returned positive, confirming the diagnosis of racemose neurocysticercosis (RNCC). He began treatment with corticosteroids followed by albendazole and praziquantel.
Discussion: Neurocysticercosis should be considered in any patient with neurological symptoms who has lived in or traveled to endemic regions, including Latin America, sub-Saharan Africa, and Southeast Asia. The latency period between infection and symptom onset can span years to decades, making remote exposure relevant. Unlikely parenchymal NCC, which classically presents with seizures, the clinical presentation of RNCC is nonspecific and can vary widely, correlating with the mass effect of the cysts and the degree of inflammatory response. In this case, the initial MRI findings of diffuse sulcal FLAIR hyperintensity with corresponding susceptibility signal represented a significant diagnostic challenge: this pattern is nonspecific and can be seen in subarachnoid hemorrhage, meningitis, leptomeningeal carcinomatosis, and inflammatory conditions. The transient nature of these findings, with resolution on repeat imaging, likely reflected the inflammatory response to cyst degeneration or intermittent antigen release, a phenomenon well-described in NCC. The subsequent identification of multiple subarachnoid cysts with a visible scolex in one lesion was pathognomonic for neurocysticercosis.
Conclusions: Racemose neurocysticercosis represents a diagnostically challenging variant of NCC that can mimic other serious neurological conditions including subarachnoid hemorrhage and chronic meningitis. Hospitalists play a critical role in the initial evaluation and stabilization of these patients and should maintain a high index of suspicion for NCC in patients from endemic regions presenting with meningeal symptoms or unexplained CNS cystic lesions.