Case Presentation: A 61-year-old man with a history of GERD, tobacco, and alcohol use presented to our hospital with a week-long exacerbation of subacute abdominal pain and constipation. He had presented multiple times in recent months to outside hospitals with similar symptoms. CT and MRI scans showed a small bowel obstruction (SBO) with a transition point, terminal ileitis, and fat stranding. An EGD was unremarkable. Colonoscopy showed an ulcer of the ileocecal (IC) valve, a non-traversable stricture at the terminal ileum, and a 5 cm polyp in the descending colon. Biopsies showed normal ileal mucosa, focal acute colitis of the IC valve, and high-grade dysplasia of the polyp. GI and general surgery were consulted, a diagnosis of Crohn’s was made, his symptoms improved with steroids, and he was discharged on a prednisone taper with GI clinic follow-up. He was unable to present to the GI clinic due to recurrence of symptoms. When he presented to our hospital, the workup was remarkable for normal ESR, CRP, B12, CMP, and CBC. CT and MRI enterography with and without contrast showed findings similar to prior evaluations. GI recommended surgical resection for a stricture deemed unresponsive to medical management. In the operating room, an obstructing mass was noted at the IC valve. Pathology showed a 4 cm invasive poorly differentiated adenocarcinoma with metastases to multiple lymph nodes and the peritoneum.
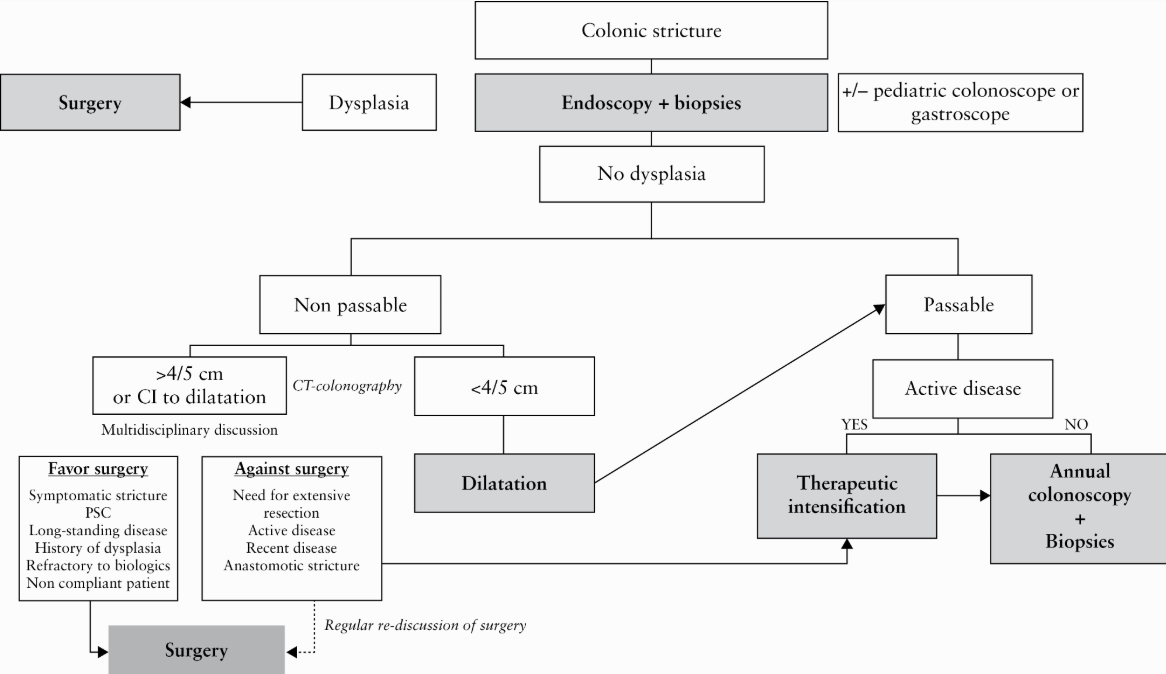
Discussion: We present a case of SBO and stricture at the IC valve, suspected to be due to Crohn’s disease, but instead found to be an IC adenocarcinoma with peritoneal carcinomatosis. This case highlights the classic diagnostic complexity that internists face when there is significant overlap in the presentation between two diagnoses, and how early closure of the differential diagnosis can lead to missed opportunities to better care for our patients. The diagnosis of Crohn’s disease relies on a combination of symptoms, radiologic, endoscopic, and pathologic findings (1). While there is significant overlap between signs and symptoms in Crohn’s disease and cancer, several factors were concerning for cancer, including his age, smoking and alcohol history, absence of prior screening colonoscopies, and no family history of Crohn’s. He had a typical Crohn’s stricture and terminal ileal inflammation, but lacked features like bloody diarrhea, malabsorption, elevated ESR or CRP, or extraintestinal manifestations. Review of prior admissions revealed a CEA of 241; while CEA can be elevated in benign conditions, it rarely exceeds 30 in such cases (2). We highlight two important points: 1] Biopsy is critical in both Crohn’s and GI cancer, but colonoscopy was limited by an impassable stricture. In stricturing Crohn’s disease, European guidelines suggest early consideration of stricture resection, especially when dysplasia is found, due to the risk of undetected neoplasia in or proximal to the stricture (3). 2] CT and MR enterography have sensitivities of 75.9% and 92.6% for small bowel neoplasms, respectively. Cancerous lesions may be missed due to overlap with benign strictures (e.g., mild or symmetric wall thickening) or loss of mural stratification from chronic inflammation or fibrosis; thus, special care needs to be taken to not rule out cancer based on prior imaging (4-6).
Conclusions: This case highlights the diagnostic overlap between stricturing Crohn’s disease and colon cancer and the heightened risk for anchoring, which in this case led to a missed opportunity to better prepare the patient for a life-altering diagnosis of cancer.