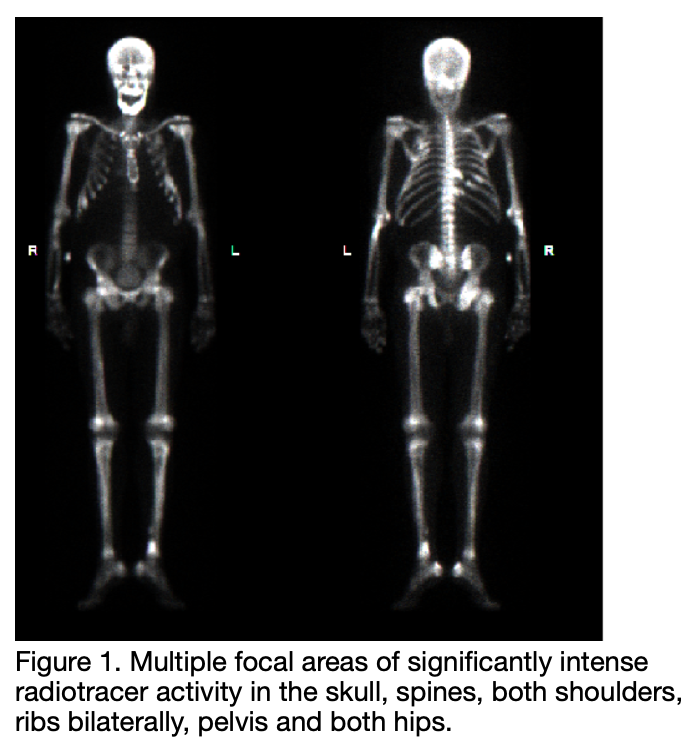
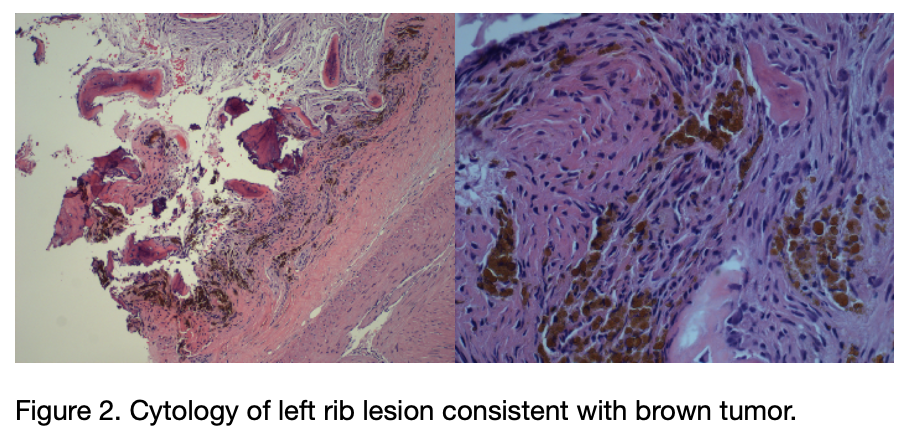
Case Presentation: 46 year old male with HTN presented to our facility with frequency, difficulty urinating and dribbling. Imaging revealed urinary retention, multiple 1mm non-obstructing renal calculi, lytic lesions in the axial skeleton, and numerous cysts within the kidneys, compatible with long standing kidney disease. Despite relief of obstruction via bladder catheterization, minimal renal improvement was noted and patient was initiated on intermittent hemodialysis. Admission serology revealed Hgb 8.5, HCO3 10, BUN 114, SCr 12.0, Phos 7.2, Ca 9.8, ALP 715 and GFR 6. Further investigations revealed hyperphosphatemia with a PTH initially 4393.7. PTH-rP was <2. He was started on a calcimimetic and phosphate binder. Multiple lytic lesions of the axial skeleton, as well as pelvis and hips were found on bone scan (Figure 1). Biopsy of left rib revealed fibrosis, bone remodeling and hemosiderin deposition, consistent with brown tumour (Figure 2). Chest CT was significant for left paratracheal soft tissue mass and subsequent biopsy revealed neoplastic follicular cells. Due to concern for malignancy, patient was referred for subtotal parathyroidectomy which revealed hyper cellular parathyroid gland. He completed 15 dialysis sessions at our facility and has not required any further in the last year.
Discussion: Brown tumor has been reported in 1.5% to 1.7% of patients suffering from secondary hyperparathyroidism (HPT) and in 4.5% of those with primary HPT [1]. Above,, we report a case of a patient with CKD who had an incidental finding of brown tumor due to secondary HPT.Brown tumor, also known as osteitis cystica fibrosa, predominantly affects clavicles, extremities, pelvis and ribs, as seen in our patient [1]. Pharmacological management such as with calcimimetics, phosphate binders and vitamin D analogues for at least 6 months are the treatment options most commonly used. However, if this fails, renal transplant or parathyroidectomy may be necessary. In our patient, due to multiple brown tumors with very high PTH and concern of malignancy, surgical management was warranted.
Conclusions: Requirement of parathyroidectomy increases linearly with duration of hemodialysis (15% after 10 years, 38% after 20 years) [2]. Interestingly, our CKD 5 patient with PTH>4300 and significant bone involvement required parathyroidectomy, despite not being ESRD. Physicians should be aware of serology and radiological findings for brown tumor in order to better recognize and initiate early treatment.