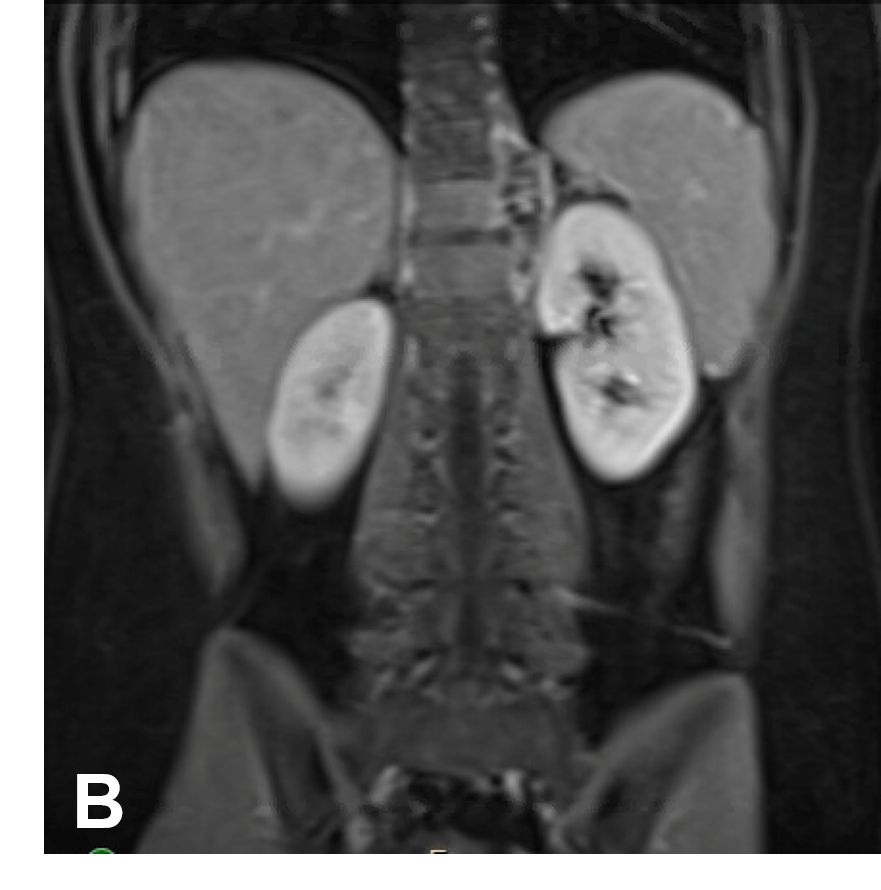
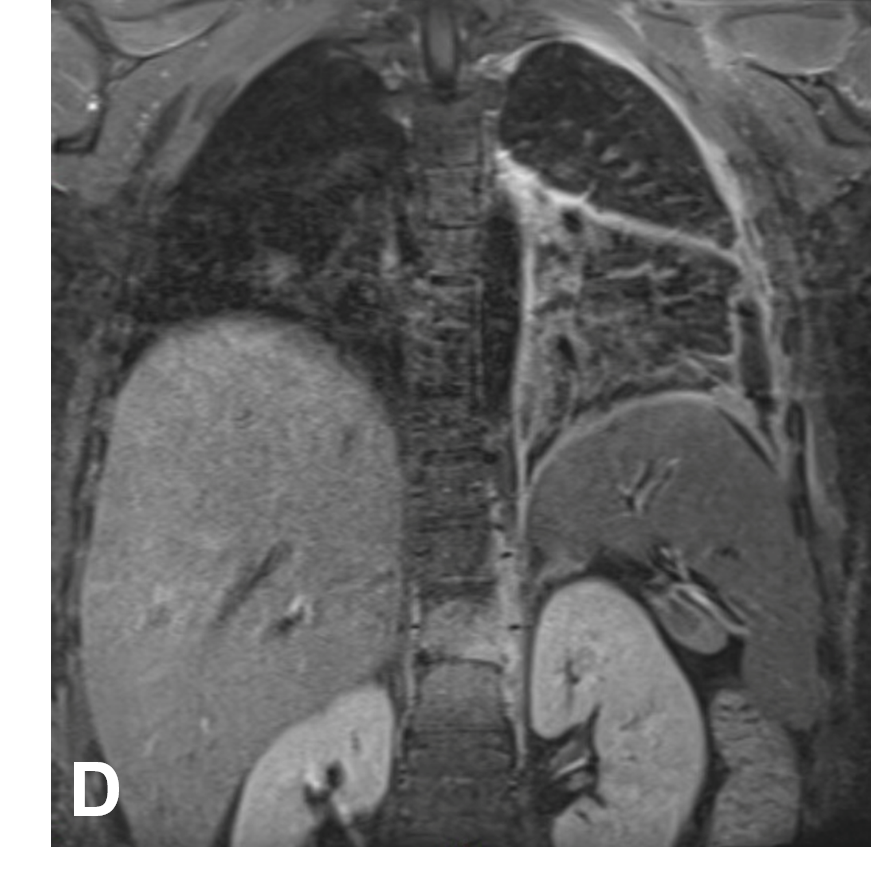
Case Presentation: A 12-year-old healthy female presented for three weeks of abdominal pain, loose non-bloody stools accompanied by night sweats and an eight-pound weight loss. Initial exam was only significant for diffuse abdominal pain. An abdominal X-ray demonstrated a unique appearing paravertebral stripe which prompted a follow up MRI abdomen/pelvis. MRI imaging revealed a 5.8 cm left paravertebral mass at T10-T12 with a radiographic differential including neuroblastoma, ganglioneuroblastoma, or lymphoma (Image 1). Subsequent vertebral mass biopsy showed histiocytic infiltrate with negative AFB stain and no malignancy on flow cytometry. The patient was discharged home with close oncology follow up. Three days later she returned with new left sided chest pain, dyspnea, and an unrelenting fever. New symptoms raised concern for a diagnosis other than malignancy, including infectious and rheumatologic. On exam the patient was ill appearing, febrile (103°F) with rigors. Lung exam had decreased breath sounds with dullness to percussion at the left lung base. There was no cardiac murmur, skin rash, or lymphadenopathy. There was tenderness to the lower thoracic vertebra but no lower extremity weakness or paresthesia. Laboratory evaluation was significant for negative blood cultures, HIV Ab and quantiferon TB test. Lung ultrasound showed complex left pleural collection prompting VATS and pig-tail catheter placement. Pleural rind culture grew non-typhoid Salmonella. Fecal Salmonella PCR was negative. MRI dedicated to the thoracic spine for ongoing fever showed T10-12 vertebral osteomyelitis with adjacent paraspinal abscess and resolving left lung empyema (Image 2). The patient responded well to a four-week course of ceftriaxone antimicrobial treatment followed by two weeks of oral cefdinir.
Discussion: We present a case of non-typhoid Salmonella gastroenteritis with hematogenous spread to the spine and pleural space in a healthy adolescent. Further history revealed the family ate meat from a local butcher prior to onset of symptoms and had self-resolved diarrhea. It is unclear if the pleural space infection was due to the primary infectious process or related to a communicating tract following needle biopsy with spread from the paraspinal infection. Salmonella is a common enteric pathogen, however, invasive multisite infection affecting either the bones or pleural space is rare in immunocompetent hosts. Pulmonary Salmonella infection is almost exclusively reported to be found in individuals with malignancy, tuberculosis or other immunocompromised states. Vague symptoms and imaging concerning for malignancy, likely resulted in anchoring bias that delayed further evaluation of infectious etiologies for her fevers.
Conclusions: This unique case of multisite salmonellosis, involving the pleural space and the vertebra, highlights the importance of maintaining a broad differential in pediatric patients with fever and contributes to a growing caseload of immunocompetent children with invasive Salmonella disease.