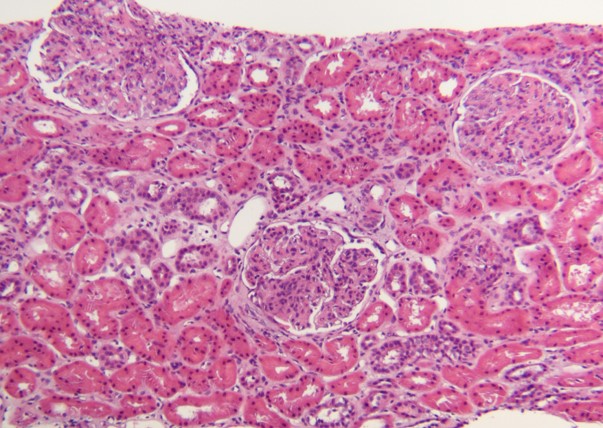
Case Presentation: A 22-year-old male with history of syringomyelia and Chiari malformation status post repair presented as a transfer for a 1-week history of fever, progressive dyspnea, reduced appetite, and headache. On his initial presentation, he was found to be hypoxic after which a chest radiography showed an enlarged cardiac silhouette. Lab work showed new onset anemia, elevated creatinine and D-dimer. Computed tomography angiography of the chest was notable for bilateral pleural effusions and a large pericardial effusion with compression of the pulmonary arteries concerning for early tamponade. An urgent pericardiocentesis yielded approximately 1 L of serosanguinous fluid with no further re-accumulation of the effusion on repeat echocardiography. Continued work up revealed elevated inflammatory markers as well as positive anti-nuclear antibodies with titers 1:1280 and positive double-stranded DNA antibodies. Upon further investigation, the patient reported recent polyarticular joint pain and swelling for the past month without any rashes, photosensitivity, oral ulcers, weight loss or family history of autoimmune disease. Hospitalization was complicated by worsening of kidney injury with urinalysis revealing hematuria and proteinuria. The patient subsequently underwent a kidney biopsy which suggested class IV classic lupus nephritis under light microscopy. Intravenous solumedrol and mycophenolic acid were started with improvement in kidney function after which the patient was safely discharged with rheumatology follow up for new diagnosis of Systemic Lupus Erythematous (SLE).
Discussion: SLE is a multisystem autoimmune disease affecting all organs of the body including the cardiovascular system. While pericarditis and pericardial effusions are two of the well-recognized sequalae of this disease, cardiac tamponade is typically a rare but life threatening initial presentation. In young patients presenting to the hospital with tamponade, it is crucial to identify the disease so that prompt treatment can be started with steroids and immunosuppressants to slow the disease progression and prevent further organ damage.
Conclusions: Cardiac tamponade is a rare initial presentation of SLE. Rheumatologic testing should be considered by inpatient providers in young patients presenting with tamponade despite absence of the typical symptoms of SLE so that proper treatment can be initiated immediately.