
Background:
Cardiorenal syndrome (CRS) occurs in 25% of patients hospitalized for heart failure and is associated with increased length of stay, readmission, and death; currently, there are no treatments with proven efficacy. We report our initial experience with slow continuous venovenous ultrafiltra‐tion (UF) using the Aquadex system 100 in hospitalized heart failure patients with CRS.
Methods:
We identified 6 patients hospitalized for heart failure and volume overload who developed worsening renal function (increase in creatinine 0.3 mg/dL from baseline) and persistent volume overload despite escalating doses of intra venous (IV) diuretics. All were treated with venovenous UF. Diuretics were held during UF, and treatment continued for each patient until clinically optivolemic.
Results:
Mean age was 60.7 years, 5 of 6 were men, and 2 of 6 had preserved systolic function. The mean peak daily dose of diuretics in IV furosemide equivalents prior to UF was 210 ± 62 mg. The mean weights at admit, UF start, and UF finish were 127.2 ± 47.1, 128.4 ± 44.4, and 118.2 ± 47.1 kg, respectively (P = .01 for change in weight from UF start to UF finish). The mean creatinine was 2.18 ± .81, 2.65 ± .63, and 1.92 ± .9 mg/dL, respectively (P = .03 for change in creatinine from UF start to UF finish.) Weight and creatinine at the these time intervals for each patient are shown in Figures 1 and 2.
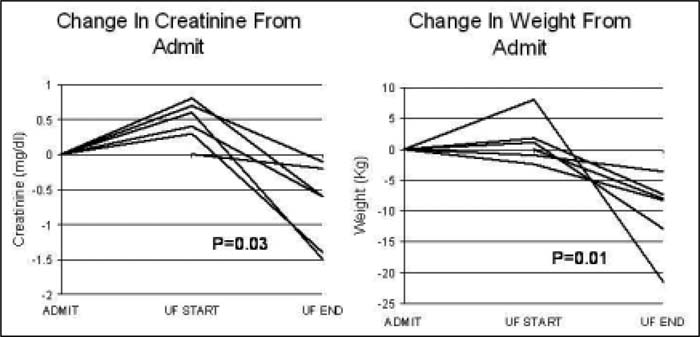
Figure 1. Figure 2
Conclusions:
Volume overload due to heart failure and subsequent CRS can be effectively treated with slow continuous venovenous UF, especially when traditional diuretic therapy is ineffective. Although only a small sample size was utilized in this study, results are promising, and it warrants further study.
Author Disclosure:
M. Walsh, none; B. Bart, none; D. Blake, none; S. Goldsmith, GSK, speakers bureau; Otsuka, research funding.