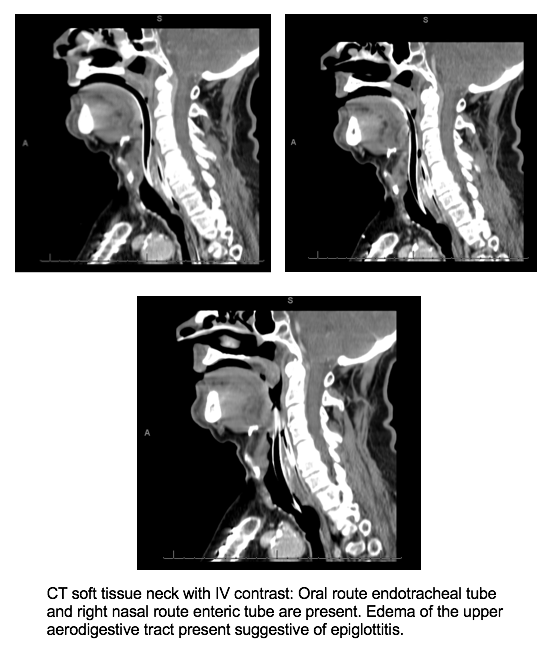
Case Presentation: A 77-year-old male with a history of coronary artery disease and hypertension presented to the emergency department with progressively worsening sore throat, difficulty speaking, and odynophagia for one day. On initial assessment, the patient was in no respiratory distress. However, with an hour of presentation, he developed respiratory distress. Examination revealed tachypnea, stridor, and hoarseness with noted desaturations in oxygen. He was subsequently intubated for impending respiratory failure. Computed tomography of the neck revealed edema of the upper aerodigestive tract consistent with epiglottitis. He received dexamethasone and piperacillin-tazobactam was empirically started. Blood cultures drawn in the emergency department grew gram-negative rods, later identified as pan-sensitive P. multocida. The patient rapidly improved with the above therapies, passing a spontaneous breathing trial, and was successfully extubated within 48 hours of intubation. Antibiotics were eventually narrowed to amoxicillin/clavulanate. Upon further questioning, he endorsed recently being scratched by a neighborhood cat, which was the suspected source of the bacteremia. He remained stable and was subsequently discharged home to complete 10 days of total antibiotic therapy.
Discussion: Epiglottitis is a rare condition in the adult population that can be life threatening without prompt recognition and intervention. Mortality rates are reported to be 1.2-7.1%. The etiology is typically infectious, with respiratory pathogens including Streptococcus pneumoniae, Staphylococcus aureus, and Haemophilus influenza being the most common causative organisms. Pasteurella multocida is an exceedingly rare and infrequently cited cause of acute epiglottitis. P. multocida, commonly found in the respiratory tract of domestic cats and dogs, is a rare cause of acute epiglottitis. Exposure to such animals has been implicated in previously reported cases of P. multocida epiglottitis, and was the case with our patient. Incidence in adults ranges from 0.97 to 3.1 per 100,000. Symptoms include rapidly worsening sore throat, dysphagia, and odynophagia, all of which were demonstrated in our patient. Blood cultures should be drawn to identify the causative organism in order to tailor appropriate antibiotic selection. The hallmark treatment is antibiotic therapy for one to six weeks, depending on the severity, and upper airway management, typically leading to rapid resolution of symptoms.
Conclusions: Acute epiglottitis can occur at any age, but it is uncommon in adulthood. We present a rare cause of epiglottitis that emphasizes the importance of both developing a broad differential and obtaining a thorough history. It is important for clinicians to be aware of the clinical manifestations of epiglottitis, as early airway management is critical.