Background: Hospitalists provide around-the-clock care for patients. There is a need to characterize the work and workflows of hospitalists during different times of the day in order to ensure that clinicians are tasked with workloads that enable safe patient care, alignment with quality goals, professional fulfillment, and efficient use of resources. While there are relatively established metrics for measuring work during day shifts, such as admissions, rounding, and discharge encounters, measuring work during non-rounding, off-hours shifts is more challenging. Based on our previous work examining daytime workflows (1), we aim to use novel measures of off-hours workload and workflows in hospital medicine in order to accurately and reliably characterize and optimize off-hours care in hospital medicine.
Methods: This study was approved by the University of Minnesota IRB. We analyzed a cohort of all patients on the adult hospital medicine service at a large, urban, quaternary care medical center in the Upper Midwest for a 6 month period. We combined user electronic health record (EHR) audit log data as well as physician scheduling data to reliably determine physicians’ activities in the EHR throughout all hours of the day; we then restricted our analysis to night work only. We used the Access Log file, which captures detailed time-stamped observations of hundreds of different tasks in the EHR. We constructed per-shift measures of EHR use, including total EHR time per shift, unique patient charts accessed per shift, number of “activated” hours for which at least some EHR activity was observed, as well as time spent on clinical notes, orders, patient clinical information, and other workflows. We divided patients into deciles based on hospitalist EHR time and examined differences between different shift types (hybrid direct care/resident supervision and hematology-oncology focused). We also examined EHR activities throughout the shift and by the night of the week.
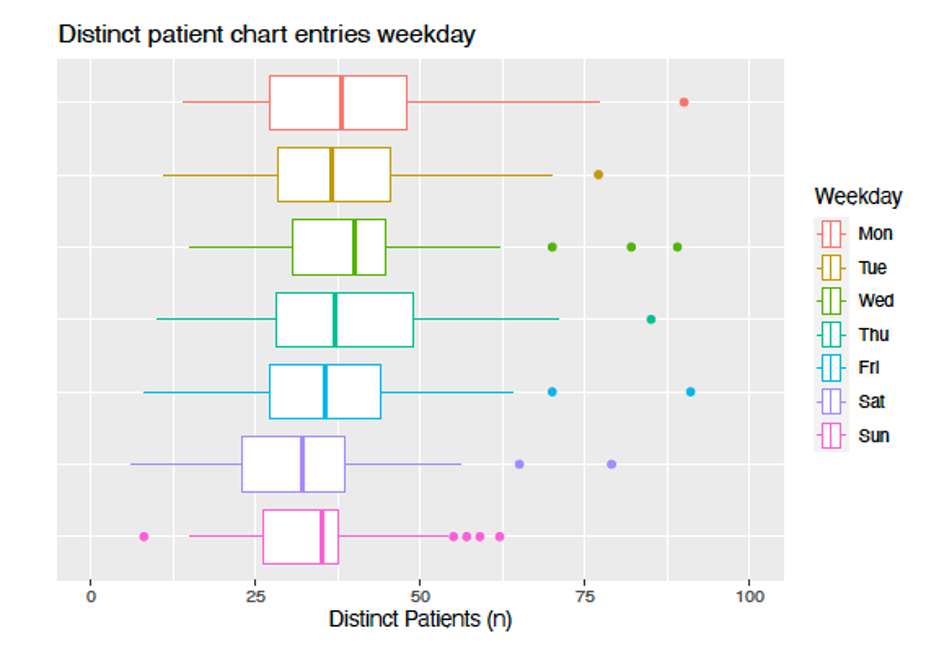
Results: 40 physicians worked 344 shifts over the 6-month period. The group of physicians accessed the charts of a total of 2964 patients, a mean (SD) of 38.49 (18.72) per shift. Physicians spent a mean (SD) of 266 (97) minutes in the EHR per shift, with significantly more time in the hybrid role vs hematology-oncology role. The top decile of patients for total EHR time accounted for a mean (SD) of 45 (12)% of hospitalist EHR time during shifts. This relationship becomes even more pronounced as the number of unique charts accessed per shift increases. (Figure 1) The number of unique charts accessed varies substantially by night of the week, with lower values on the weekend, although total EHR time does not. (Figure 2) Lastly, the patterns of EHR work vary between the two shift types.
Conclusions: Our findings show that hospitalists spend a significant amount of time in the EHR at night and spend more time in the EHR than their daytime colleagues, accessing nearly three times as many unique charts. Given that a small number of patients account for most EHR time, there may be an opportunity to change patient assignments to level-load. In addition, there appears be be work compression happening as more charts are accessed with implications for cognitive load (2) and potentially patient safety. Given workflow pattern differences between shifts, there appears to be an opportunity to improve teamwork to take advantage of peaks and valleys in activity throughout the shifts. Future work should link these analyses to hospitalist engagement as well as patient and hospital-level outcomes.