Background: Paracentesis is associated with decreased mortality in patients with advanced liver disease. The prevalence of paracentesis related complications is not well characterized, but prior studies suggest improved safety outcomes when ultrasound guidance is employed. The Agency for Healthcare Research and Quality utilizes patient safety indicator (PSI) 27 to identify postoperative bleeding complications. Our aim was to use PSI 27 codes and validated renal codes to comprehensively assess the prevalence of paracentesis-related complications via the Nationwide Inpatient Sample (NIS), an all-payer database of discharge data representing a 20% sample of hospitals in the US.
Methods: We queried the NIS to select hospitalized patients between 2004-2012 with a primary diagnosis of ascites, spontaneous bacterial peritonitis, or hepatic encephalopathy (HE). All patients had a secondary diagnosis of cirrhosis. Patients with HE had a secondary diagnosis of ascites. Our independent variable was procedure coding for paracentesis (ICD9 54.91). Outcomes included procedure-related bleeding complications, acute kidney injury (AKI), incident renal replacement therapy (RRT), and mortality.
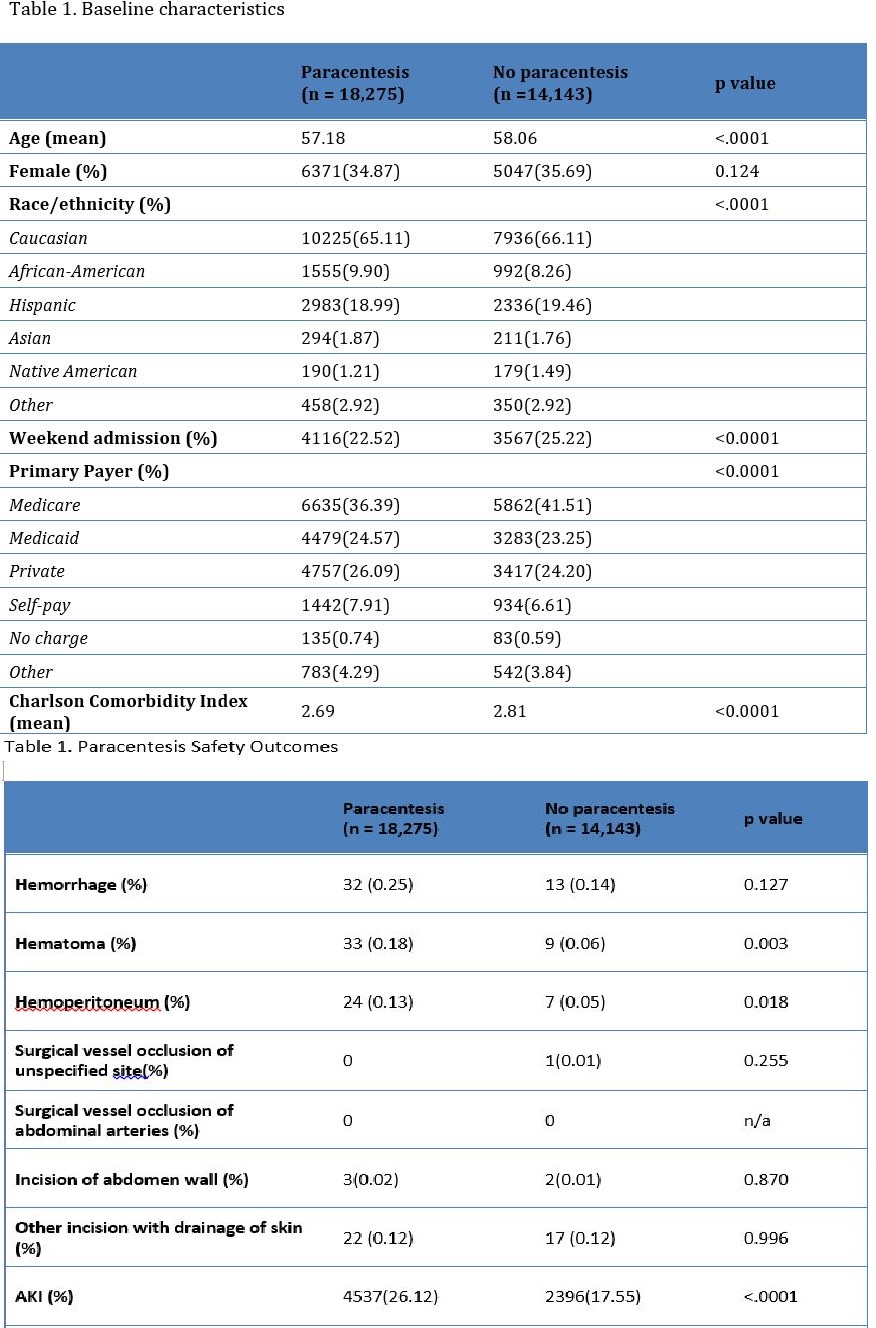
Results: 32,418 patients met inclusion criteria; 18,275 (56.37%) received paracentesis. There was a 10% increase in patients receiving paracentesis from 2004 (50.16%) to 2012 (60.77%; p<.0001). Mortality was lower in patients undergoing paracentesis (6.37% vs 8.09%, p<0.0001). Identified paracentesis bleeding complications were abdominal hematoma (0.18% vs. 0.06%; p= 0.003) and hemoperitoneum (0.13% vs. 0.05%; p=0.018). Adverse renal outcomes were more common in patients undergoing paracentesis (AKI 26.12% vs. 17.55%; p<.0001 and RRT 1.84% vs 1.20%; p<0.0001). LOS was higher in patients receiving paracentesis (6.63 vs. 5.31 days; p<.0001). In acuity adjusted multivariable models, the mortality benefit of paracentesis persisted but was slightly attenuated by the presence of AKI.
Conclusions: Our study confirmed a mortality benefit from paracentesis in hospitalized patients eligible for paracentesis, and this benefit became more pronounced over time. Although underutilized, paracentesis has become more prevalent in recent years. The increasing use of ultrasound guided paracentesis may explain both of these findings – ultrasound guidance should be employed whenever possible. Although bleeding complications from paracentesis were rare, codes for abdominal hematoma and hemoperitoneum may be suitable safety metrics. In contrast, adverse renal outcomes are common, more frequent in patients undergoing paracentesis, and may attenuate the mortality benefit of paracentesis. Hence, the prevention of post-paracentesis AKI is a suitable target for safety improvement.