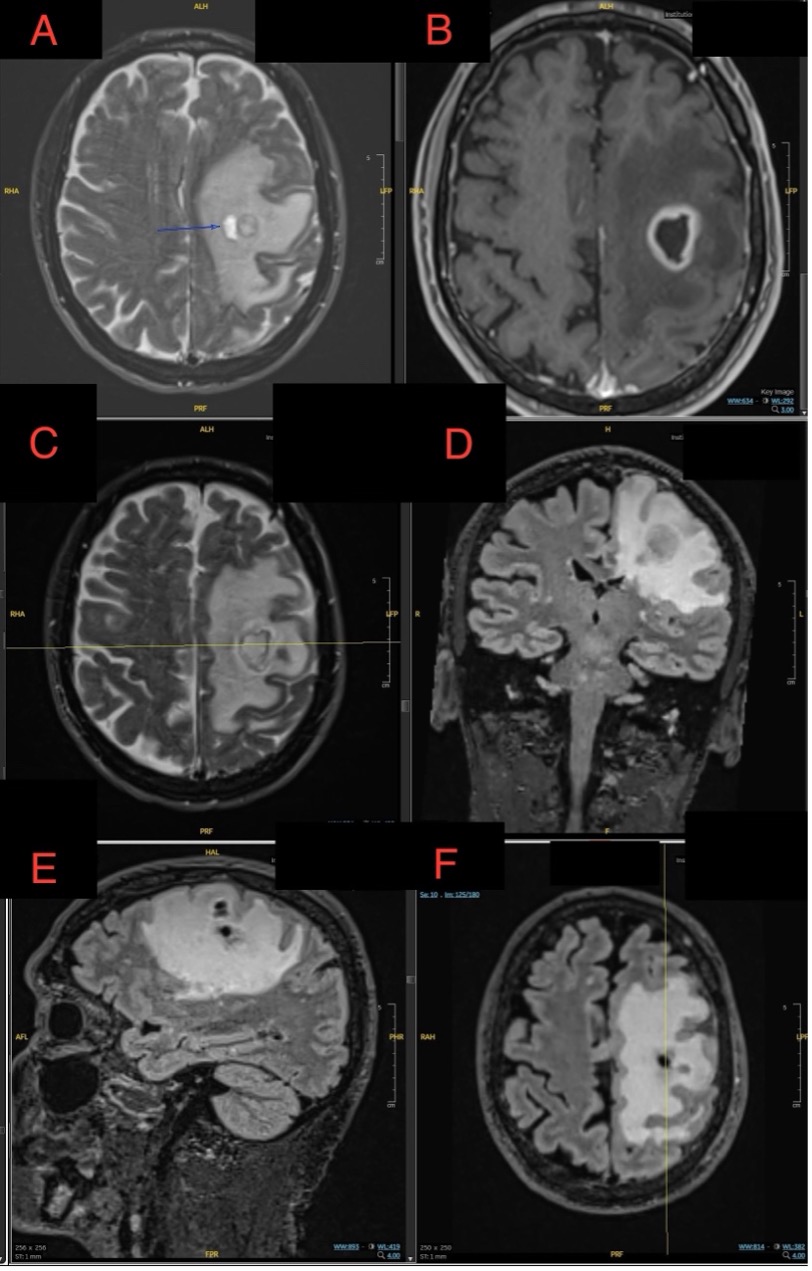
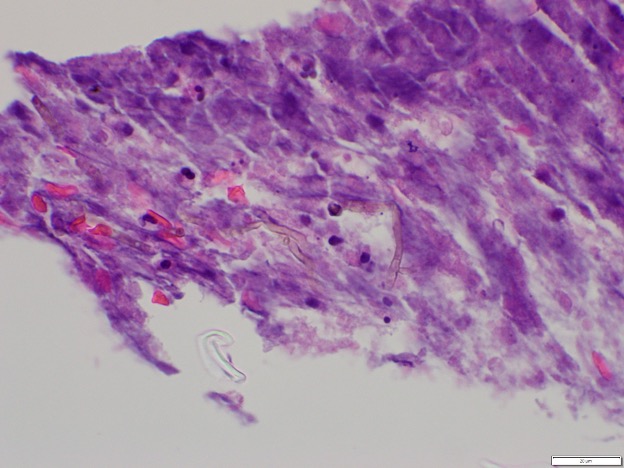
Case Presentation: A 73-year-old male with hypertension, hyperlipidemia, and mild COPD presented with word-finding difficulties. Initial brain imaging at an outside hospital suggested a left intra-axial peri-Rolandic lesion, raising suspicion for a primary brain tumor like glioma. He was transferred for neurosurgical evaluation, where MRI revealed a ring-enhancing lesion with restricted diffusion, consistent with a brain abscess. A stereotactic brain biopsy confirmed a fungal abscess caused by Cladophialophora species.Further evaluation with a chest CT scan showed a nodule with a halo sign in the right lung and a ground-glass opacity in the left lung. These findings were concerning for fungal dissemination but had resolved by the time of the brain abscess diagnosis, making the relationship to the brain infection uncertain. The patient was treated with voriconazole, steroids, and levetiracetam for seizure prophylaxis. He demonstrated significant neurological improvement, regaining strength in his right side from 2/5 to near-complete recovery. He was discharged to a skilled nursing facility with plans for follow-up care, including repeat MRI.
Discussion: This case illustrates the diagnostic challenge of distinguishing fungal brain abscesses from primary brain tumors like gliomas based on imaging alone. The initial presentation and radiographic findings mimicked malignancy, underscoring the importance of maintaining a differential diagnosis that includes infectious etiologies, particularly for lesions that present with ring enhancement. Stereotactic biopsy was crucial for establishing the diagnosis, emphasizing its role in cases where imaging alone cannot definitively differentiate between abscess and tumor.The transient pulmonary findings highlight the potential for fungal dissemination from the lungs to the CNS, even without persistent lung lesions, and stress the importance of thorough evaluation for possible entry points in systemic infections. This is particularly relevant for Cladophialophora, known for its neurotropic tendencies and capacity to infect immunocompetent individuals. Treatment with voriconazole, an antifungal with good CNS penetration, proved effective in this case, but outcomes are often poor without early intervention, with reported mortality rates up to 70%.
Conclusions: This case emphasizes the importance of considering infectious causes in brain lesions, even when imaging suggests malignancy. A high index of suspicion, timely biopsy, and appropriate antifungal treatment are critical for improving outcomes in rare and potentially fatal CNS infections like Cladophialophora brain abscesses. Multidisciplinary collaboration is essential in managing such complex cases effectively.