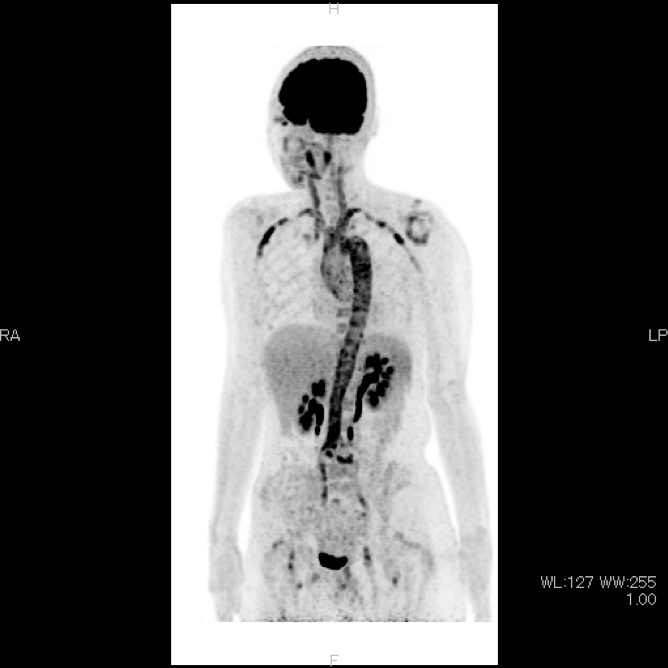
Case Presentation: A 57-year-old Japanese woman with a history of atopic dermatitis and recurrent cystitis presented to our hospital with a 4-week history of intermittent fever with chills, unlocalized mild headache, appetite loss, and 6-kg weight loss. Four weeks earlier, she developed fever without any localized symptoms, except for a mild headache. Her symptoms did not improve despite serial oral antibiotic treatments for a presumed urinary tract infection; hence, she was referred to our hospital for further evaluation. Previously, she had not experienced similar episodes and she did not have any family history of periodic fever syndrome. The patient denied recent travel, sexual activity, animal exposure, or sick contact. She had no skin rash, arthralgia, vision change, chest pain, abdominal pain, jaw claudication, and upper and lower extremity claudication. On her first visit, she appeared chronically ill, but was not in acute distress. Her vital signs were BT 36.4℃, HR 86, BP 120/68, RR 18, and SpO2 97% in room air. Physical examination revealed that there was no lymph node swelling, hepatosplenomegaly, skin rash, or arthritis. No carotid bruit and diminished peripheral pulses were noted. The laboratory tests were only notable for nonspecific inflammatory responses—C-reactive protein level: 9.55 mg/dL, ESR: 82 mm/hr, and Hgb level: 10.3 g/dL(MCV 82 fl)—and repeat blood culture tests were negative. Infectious serologies and autoantibodies, including rheumatoid factor, antinuclear antibody, and anti-neutrophil cytoplasmic antibodies, were negative. Computed tomography revealed a possible slight thickening of the aortic wall, which was noncontributory. Further imaging with positron emission tomography-computed tomography (PET-CT) demonstrated diffuse, intense fluorodeoxyglucose uptake in the thoracic and abdominal aorta, common carotid arteries, subclavian arteries, iliac arteries, and femoral arteries, consistent with large vessel vasculitis. Doppler ultrasonography of the large vessels revealed no signs of vascular stenosis. She was diagnosed with Takayasu’s arteritis (TA), and treatment was initiated with 25 mg (0.5 mg/kg) of oral prednisolone per day. Her fever, headache, serum C-reactive protein level, and ESR gradually improved, and the prednisolone dose was successfully tapered over 16 months, without any recurrences.
Discussion: TA, also known as “pulseless disease,” is a type of granulomatous large vessel vasculitis that predominantly involves the aorta and its proximal branches. TA is more common among young females, especially Asians. Clinically, TA can be divided into systemic and subsequent occlusive phases. Early diagnosis of TA is particularly important to prevent irreversible vascular stenoses, aneurysms, or occlusions. However, the non-specific systemic signs and symptoms of TA during the systemic phase present diagnostic challenges. Recently, the clinical usefulness of PET-CT for the early diagnosis of TA have been increasingly reported. PET-CT can be more sensitive than contrast-enhanced CT in diagnosing active vasculitis, even in the early phase of TA.
Conclusions: We encountered a case of early-phase TA in a middle-aged woman with nonspecific symptoms, which was successfully diagnosed using PET-CT. PET-CT can be a sensitive diagnostic tool for febrile disease without specific presentations by excluding malignancies and depicting active vasculitis.