Background: Hospital readmissions continue to remain prevalent despite their negative impact on patient outcomes and economic cost. One in five Medicare beneficiaries is expected to be readmitted within 30 days. As a result, strategies to reduce readmissions is a point of emphasis for all healthcare systems. Guidance regarding reducing readmissions differs and is not abundant. Data shows that the process is complex and appears to require interventions at multiple levels of the process. Through integration of information technology and improved communication between Emergency room physicians and hospitalists we aimed to avoid unnecessary readmissions and identify patients who could safely be discharged home.
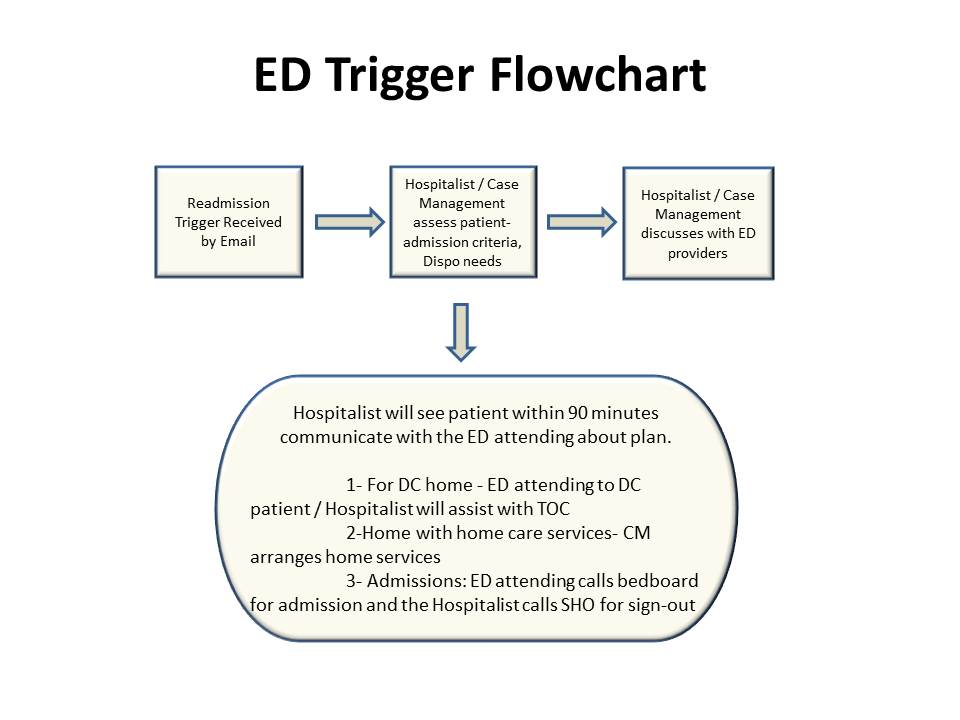
Methods: An email alert was created when a patient who was discharged from the hospitalist service within 30 days was re-registered in the Emergency room. This email was sent to the hospitalists and the Emergency room staff. The previous admission was reviewed by the hospitalist while the ED physician assessed the acute complaint. Communication between the Emergency room physician and hospitalist was to occur within 90 minutes of patient arriving to Emergency room. The discussion involved patient’s previous admission, discharge plan, current complaint and potential need for inpatient care. Through collaboration between inpatient and outpatient providers along with case management a safe plan for the patient’s care was executed.
Results: During a 45 day period a total of 146 patients met the 30 day criteria. 67% of the patients were not readmitted to the hospital and were safely discharged from the Emergency room. Of the 33% that were readmitted, we found that close to half of the readmissions were patients with active malignancy. Common etiologies for admission in this subsection of patients were uncontrolled pain, failure to thrive, worsening of malignant disease or chemotherapy related side effects. A quarter of the readmissions were due to non medical reasons and on average the 30 day readmissions returned within 19 days.
Conclusions: Hospitalization is the most expensive medical decision made by a physician and often hospitalists and Emergency room physicians are the ones making these choices. Despite having similar work schedules and often being the only attending physicians in house collaboration among the two groups is not prevalent. By working together as a team we were able to decrease hospitalist readmissions as well as increase ED efficiency via decreasing boarding time. In order for hospitals to remain efficient in a diagnosis related group model of payment improved partnership between the two groups is inherent. Through teamwork we can improve safety, quality and ultimately patient care.