Background: In the US, 30-day hospital readmissions remain a significant challenge, impacting patient outcomes and healthcare costs. While conventional binary classification models predict whether readmission occurs within 30 days, survival models can capture time-to-readmission dynamics and provide time-dependent risk estimates. We compared these approaches to characterize readmission patterns and guide tailored interventions.
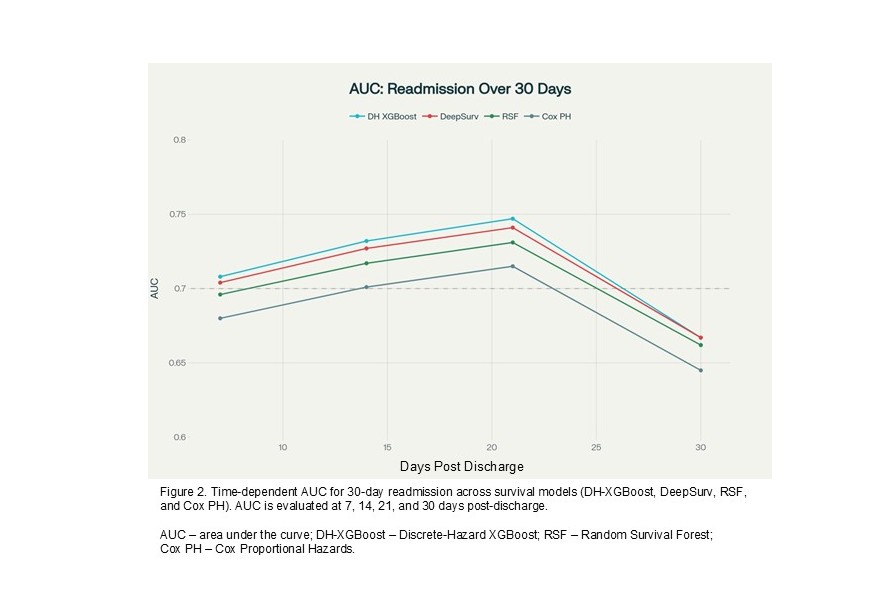
Methods: This was a retrospective cohort study of 504,654 hospital admissions (305,294 unique adults) at an institution’s 19 sites across four US states (Arizona, Florida, Minnesota, Wisconsin), from 2017‒2024. We used 203 predictors including demographics, comorbidities, vital signs, laboratory values, and medications. For binary classification of 30-day readmission, we used XGBoost with patient-level stratified grouped nested cross-validation (outer 5-fold for performance estimation, inner 3-fold for hyperparameter tuning) using precision-recall area under curve (PR-AUC) as the tuning metric with F1-optimized thresholds. We compared AUC with currently used LACE+ index. For survival analysis, we used 70-10-20 train-validation-test split to predict readmission in weekly intervals: 0‒7, 8‒14, 15‒21, and 22‒30 days using: 1) discrete time hazard XGBoost using person-period data expansion; 2) DeepSurv neural network; 3) Random Survival Forest; and 4) Cox proportional hazards (PH). We reported AUC, PR-AUC, Brier score (for accuracy), F1 (for performance in classification), C-index (equivalent to AUC) with 95% CI.
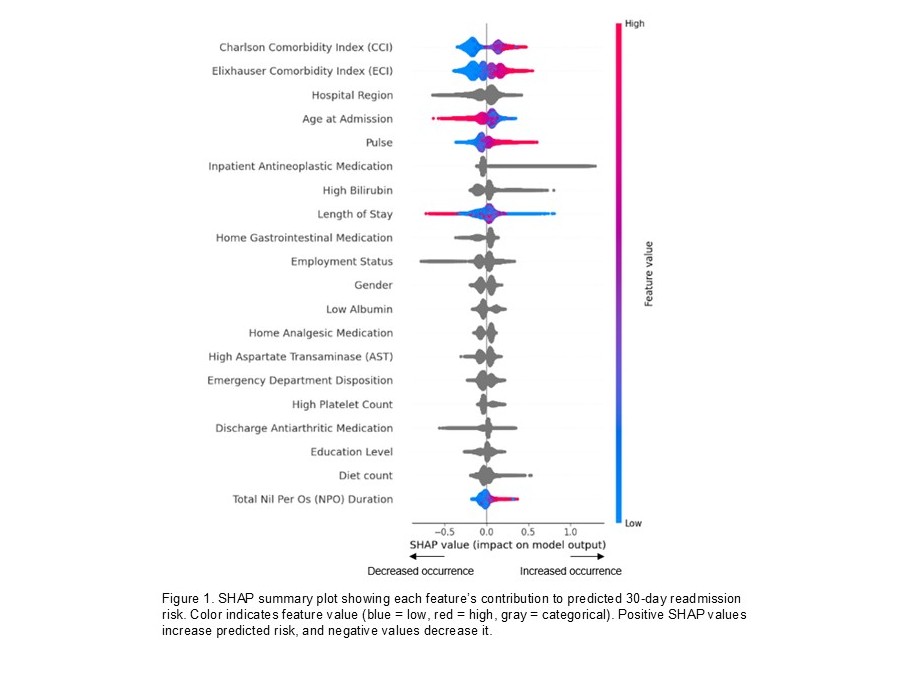
Results: The cohort had mean (±SD) age of 59.2 (±18.4) years with 50.9% female, and 30-day readmission rate of 12.7%. Predictors common to both binary classification and survival analysis included antineoplastic, cardiovascular, anti-viral, anti-fungal, and immunosuppressive medication; elevated bilirubin and aspartate transaminase (AST); low albumin and potassium; and comorbidity burden. The binary XGBoost model had an AUC 0.757 (0.756‒0.759) vs. 0.640 for LACE+, PR-AUC 0.341 (0.333‒0.349) vs. 0.191 for LACE+, Brier score 0.098 (0.097‒0.099), and F1-score 0.377 (0.372‒0.382). Among survival models, the discrete time hazard XGBoost had the highest performance (C-index 0.732 with 95%CI 0.730-0.735) and mean time-dependent AUC (0.714). Time-dependent AUC showed optimal discrimination at 21 days (AUC 0.747) with decline at 30 days (AUC 0.667), revealing temporal patterns in prediction accuracy. DeepSurv (C-index 0.731 with 95%CI 0.727-0.734), Random Survival Forest (C-index 0.723 with 95%CI 0.717-0.729), and Cox PH (C-index 0.70 with 95%CI 0.702-0.713) showed lower but acceptable discrimination. DeepSurv model demonstrated excellent risk stratification, with an 8.93-fold higher readmission in the highest-risk (27.0%) compared to the lowest-risk (3.0%) quartile.
Conclusions: Both binary classification and survival models outperformed LACE+ in predicting 30-day readmission. Binary XGBoost model provides optimal point-in-time 30-day risk prediction, while survival models offer optimal time-dependent risk trajectories with the discrete time hazard XGBoost achieving optimal balance. The binary model identifies highest-risk patients for resource allocation, whereas survival models may inform the timing and intensity of post-hospital interventions. To our knowledge, this is the first study to predict hospital readmission using weekly intervals, with the potential to be more informative for designing interventions.