Background: Renal dysfunction is a complication in patients with decompensated cirrhosis. Due to the potential morbidity and mortality of these disorders in cirrhotic patients, it is important to ensure accurate clinical measurements of renal function. Standard creatinine-based estimated glomerular filtration rate (eGFR) equations have proven to be inaccurate in cirrhotic patients, as these patients have impaired metabolic processes resulting in lower baseline creatinine levels. This overestimates GFR providing a false interpretation of true renal function. Newer eGFR formulas, Royal Free Hospital (RFH) and Glomerular filtration Rate Assessment In Liver disease model (GRAIL), have shown promise in providing more accurate assessment of renal function compared to creatinine based eGFR formulas such as MDRD-4.This case study reviews the standard “one size fits all” model of creatinine-based GFR estimation of renal function for patients with cirrhosis. By comparing RFH and GRAIL to our current hospital system’s MDRD-4 creatinine based formula, we will determine if the methods differ as it relates to the severity of renal injuries in patients with cirrhosis.
Methods: This paper compares the creatinine based MDRD-4 eGFR currently used in our hospital system to the eGFR using RFH and GRAIL formulas for a 41 yo female patient with Child C, MELD-Na 27 cirrhosis who has received a total of 100 large volume paracentesis from 2016-2019 using mean, median, standard deviation, t-scores and p-values.
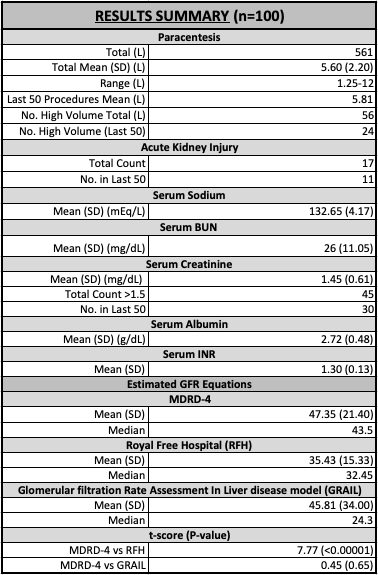
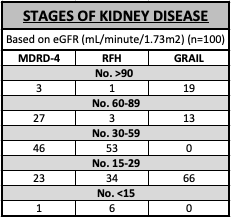
Results: The patient had a total of 561L removed via paracentesis over 3 years. She had 17 acute kidney injuries (AKI) measured across all 100 paracentesis; 11 (65%) in the last 50 procedures. In total, 45% of her serum creatinine recordings were >1.5 mg/dL with 30 (60%) in her last 50 paracentesis. Her mean eGFR from MDRD-4, RFH and GRAIL were 47.35 (SD 21.40), 35.43 (SD 15.33) and 45.81 (SD 34.00), respectively. eGFR mean measured by MDRD-4 differed from RFH by 11.92 (t-score 7.77, P<0.00001); and by 1.539 compared to the GRAIL formula (t-score 0.45, P=0.65). There were differences in kidney disease staging based on eGFR. MDRD-4 calculated that 46% of her total 100 eGFR values were between 30-60 mL/minute/1.73m2 while RFH and GRAIL were 53% and 0%, respectively. In addition, MDRD-4 showed 23% of eGFR values were between 29-15 mL/minute/1.73m2, while RHF and GRAIL calculated 34% and 66%, respectively. MDRD-4 calculated 1% eGFR value <15 mL/minute/1.73m2, while RHF and GRAIL calculated 6% and 0%, respectively. Calculating the eGFR for the patient’s last 50 paracentesis procedures using all 3 formulas, 71% of her eGFRs (17 out of 24) were <30 mL/minute/1.73m2 using MDRD-4, 73% (29 out of 40) for RFH and 62% for GRAIL.
Conclusions: eGFR differs significantly between our hospital system’s MDRD-4 and RFH, but no difference exists in MDRD-4 as compared to GRAIL. In conjunction with other studies this strongly suggests overestimation of eGFR by MDRD-4. Clinicians should consider using the RFH formula as a more accurate measure of renal function in patients with cirrhosis. Overall, this patient’s renal function declined during the last 50 procedures. This case review highlights how renal function is impacted in liver cirrhosis, and how measurements vary across eGFR calculations, thus providing clinicians with alternative means of evaluating these individuals.