Background: The 2014 ACC/AHA Perioperative Guidelines suggest using the Revised Cardiac Risk Index (RCRI), myocardial infarction or cardiac arrest (MICA), or American College of Surgeons (ACS)-NSQIP calculators for combined patient-surgical risk assessment. Alrezk and colleagues recently published a new geriatric-sensitive cardiac risk index (GS-CRI) to predict MI or cardiac arrest in the geriatric population. We recently published data comparing the performance of RCRI, MICA and ACS-NSQIP calculators in a cohort of 663 patients undergoing noncardiac surgery. However, the performance of GS-CRI has not been validated externally.
Methods: : We retrospectively analyzed a subset of patients aged ≥ 65 years old (n= 299) from our cohort of 663 patients seen in our preop clinic who underwent various intermediate-high risk noncardiac surgeries. We calculated scores for the risk indices/calculators including the new GS-CRI and recorded in-hospital and 30-day cardiac complications (MI, cardiac arrest, pulmonary edema). These scores were then compared based on predicted and observed complications.
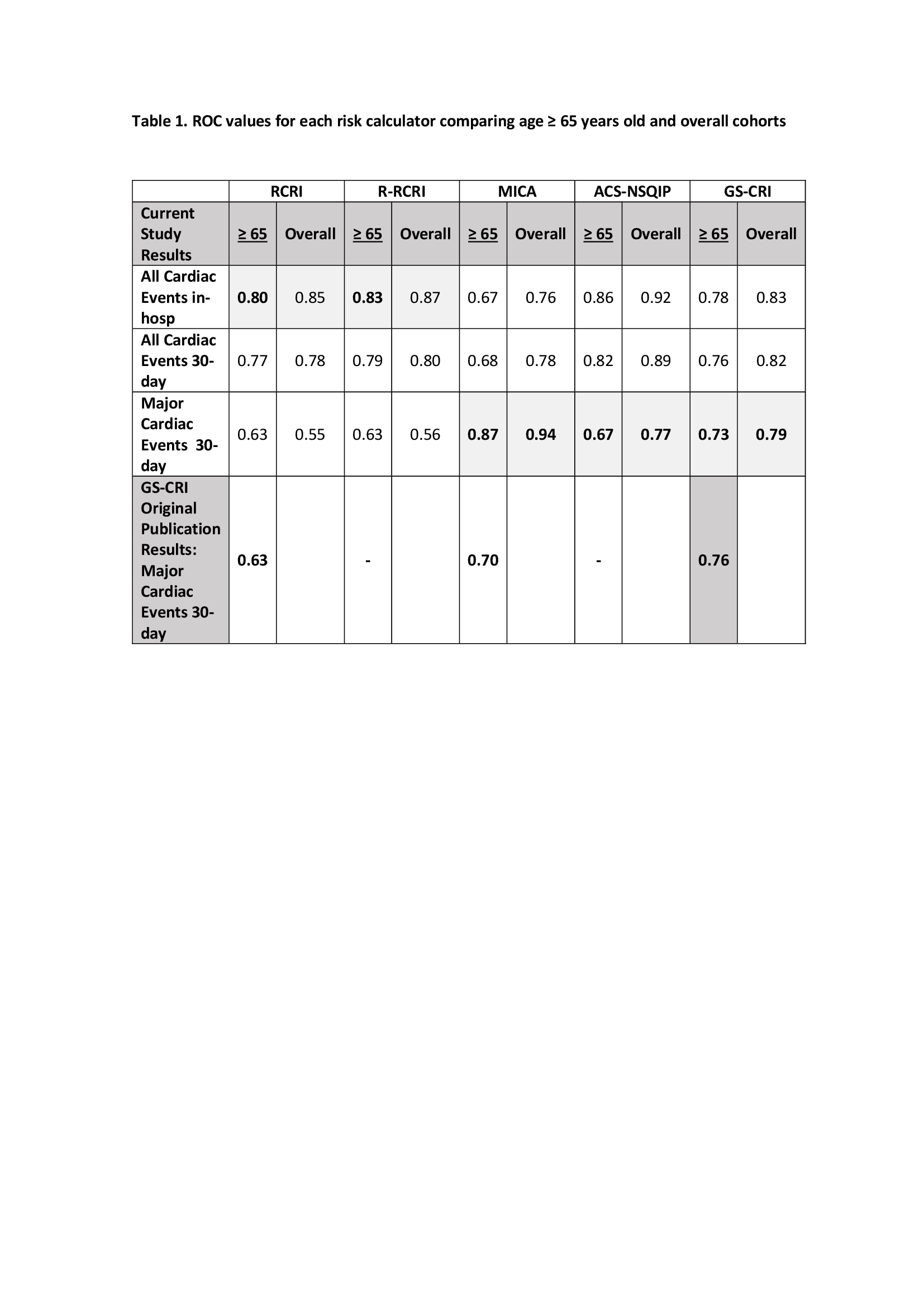
Results: 12/299 (4.0%) of patients developed cardiac complications of which 10 occurred during hospitalization. This percentage is almost 8 times higher than in patients < 65 years old in our cohort. For predicting complications as defined in the original publications, in patients ≥ 65 years old ROC curves for RCRI and Reconstructed RCRI were 0.80 and 0.83 for in-hospital complications (overall cohort AUC, 0.85 and 0.87, respectively) and 0.87 and 0.67 for MI/cardiac arrest within 30 days for MICA and ACS-NSQIP respectively (overall cohort AUC, 0.94 and 0.77). The specific risk index AUC developed for geriatric population (GS-CRI) was 0.73 (overall cohort AUC 0.79). All calculators, including the GS-CRI, performed worse in the geriatric subset than in the overall cohort. In this population, the ROCs for all risk calculators in our study were similar to values in the study of Geriatric-Sensitive CRI, except for MICA calculator which outperformed scores from all the calculators. The AUC of RCRI and R-RCRI decreases notably (∆ 17 and 20, respectively) when used to predict only major cardiac events (MI and cardiac arrest) 30 days after surgery rather than during hospitalization only and including pulmonary edema.
Conclusions: All four risk calculators performed well in the geriatric population (≥ 65 years old) especially when used to predict what they were designed to do (predict in-hospital MI, VF/CA, pulmonary edema and CHB in patients undergoing major noncardiac surgery in the case of RCRI and R-RCRI and predict MI and cardiac arrest 30-day after surgery in the case of MICA, ACS-NSQIP and GS-CRI).
One limitation of our study was the low incidence of cardiac complications, and future studies should evaluate a larger database to better define any differences between these risk calculators in the geriatric population.