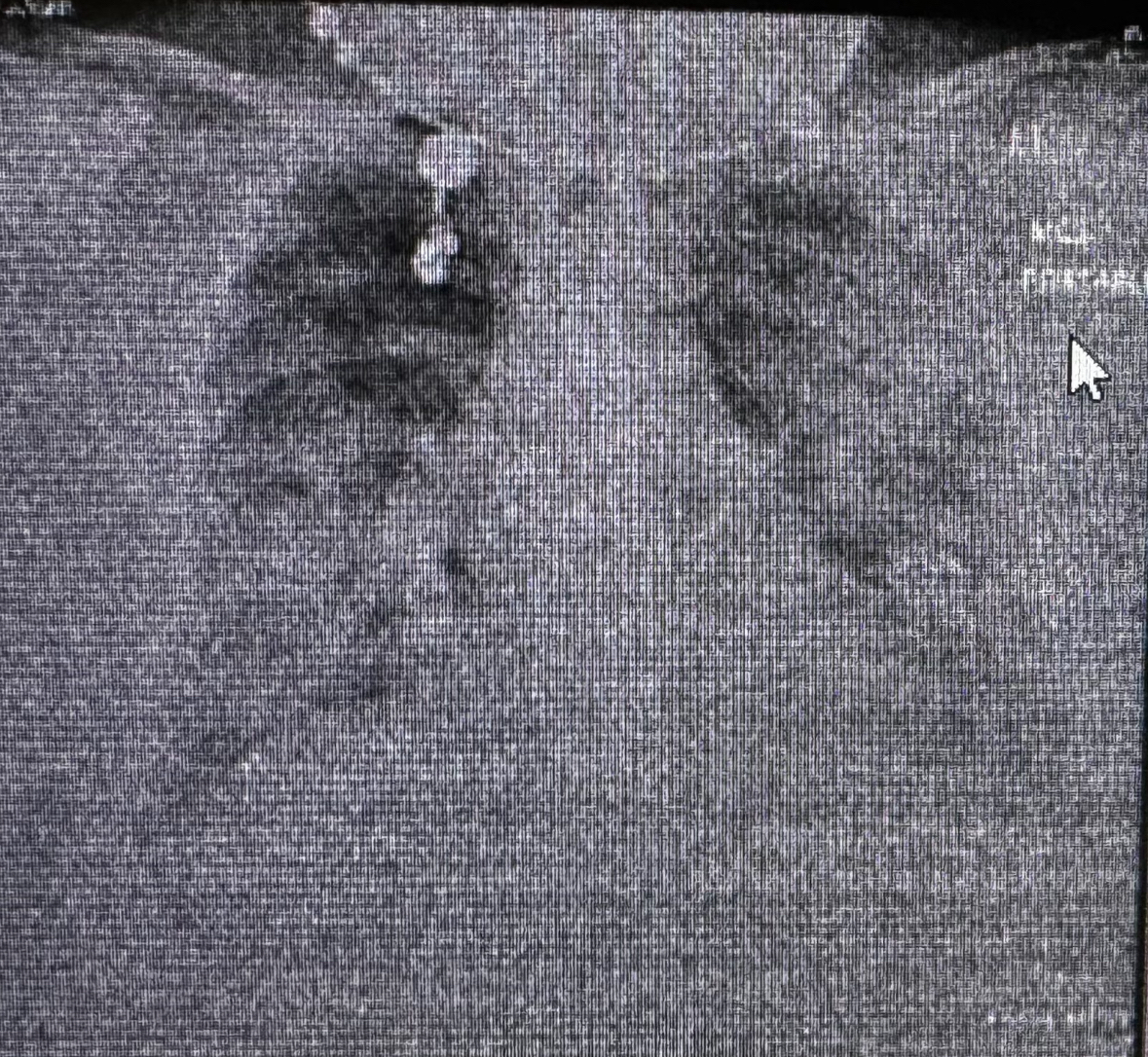
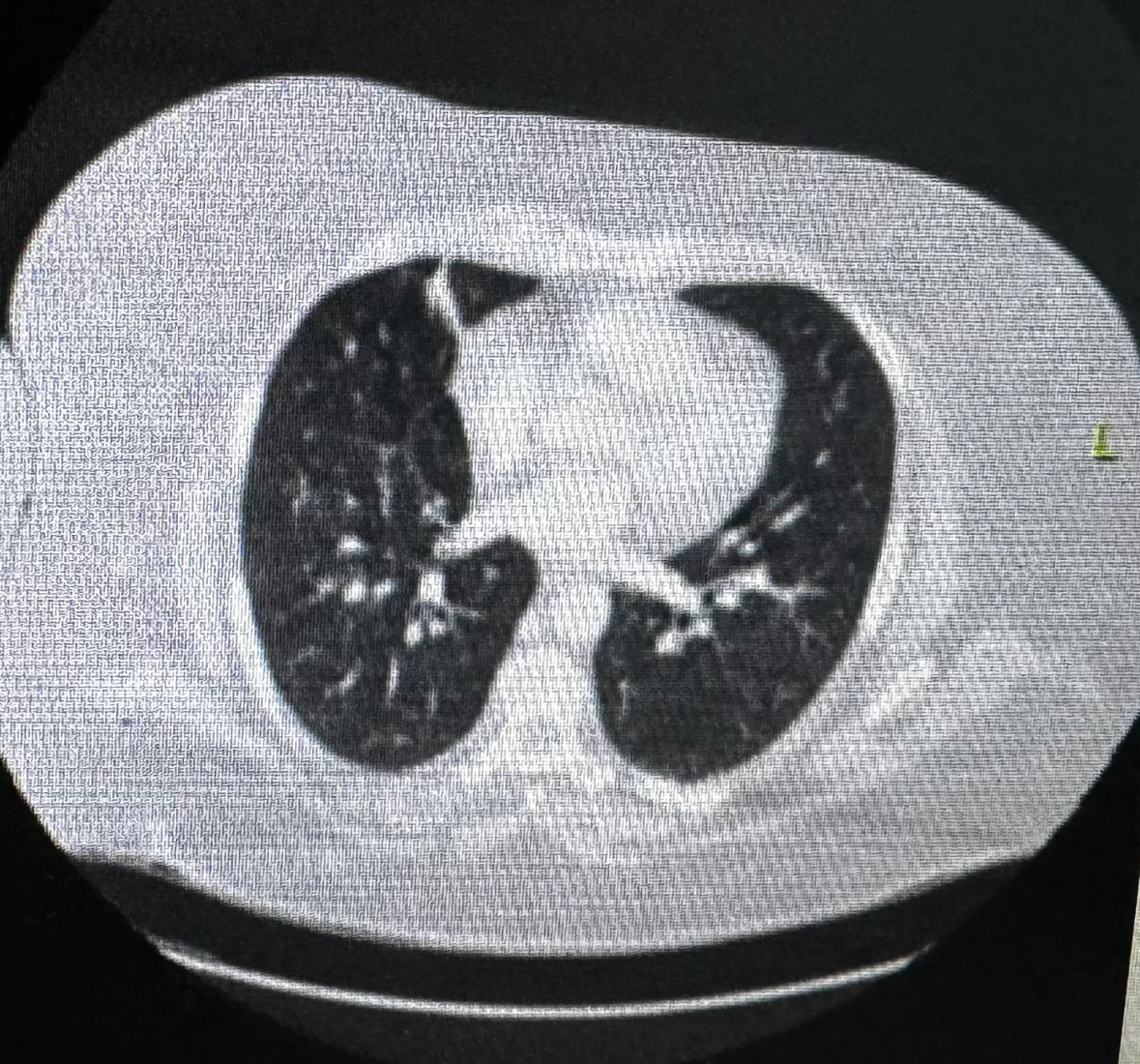
Case Presentation: A 43-year-old African-American ex-smoker with a history of biopsy-proven multisystem sarcoidosis in remission, morbid obesity, and pulmonary hypertension presented with left lower quadrant pain and was found to have multiple ventral hernias containing bowel loops without any obstruction on CT scan, following which she was discharged with outpatient surgery follow-up. Prior to contrast administration, she was pre-treated with Benadryl due to a documented contrast allergy listed as “sneezing.” Later that day, she presented with severe shortness of breath, presenting with hypoxia, tachypnea, tachycardia, with a chest X-ray showing bilateral pulmonary infiltrates, while point-of-care ultrasound showed B-lines and normal contractility of the heart. Initial labs showed elevated lactate, normal blood gases, and brain-natriuretic peptide. She was treated with IV furosemide, but she developed hypotension, prompting suspicion of contrast-induced anaphylaxis. Treatment included IM epinephrine, steroids, and bilevel-positive airway pressure (BIPAP) support, yielding some improvement, followed by an epinephrine drip and a lower dose of furosemide. Quickly, she was weaned off BIPAP and pressors in 24 hours.
Discussion: Initially, the patient was treated for congestive heart failure with diuresis. However, persistent respiratory distress, euvolemic status, hypotension, and documented mild allergic reaction (though pre-treated with Benadryl) raised suspicion for contrast-induced flash pulmonary edema. Severe contrast reactions requiring hospitalization are rare (0.004%) [1], with pulmonary edema being even rarer (0.001%-0.008%) but potentially life-threatening, underscoring the need to understand pathophysiology. This case underscores the importance of understanding the pathophysiology, hypothesized to involve vasodilation and increased permeability causing alveolar edema [2]. Notably, vasodilators like furosemide, which transiently dilates vessels, may worsen respiratory distress in already pre-dilated vessels initially, as observed in our patient.
Conclusions: The dichotomy between cardiogenic pulmonary edema (CPE) and non-cardiogenic pulmonary edema (NCPE) is a diagnostic challenge due to overlapping features and differing management strategies. Misidentification can result in severe respiratory distress and mismanagement. In this case, despite pre-treatment with anti-histamines, the patient experienced an anaphylactic reaction causing profound vasodilation. This highlights the importance of considering pre-treatment with both steroids and antihistamines when appropriate. Additionally, avoiding vasodilatory agents is crucial when vasodilation is suspected. This case highlights a rare complication, emphasizing the importance of recognition, treatment, and understanding its potential pathophysiology.