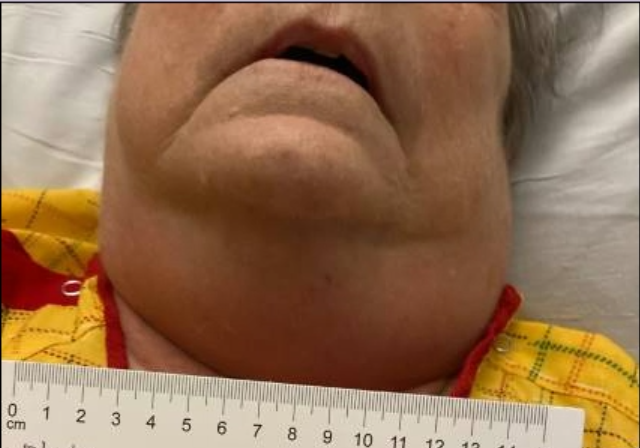
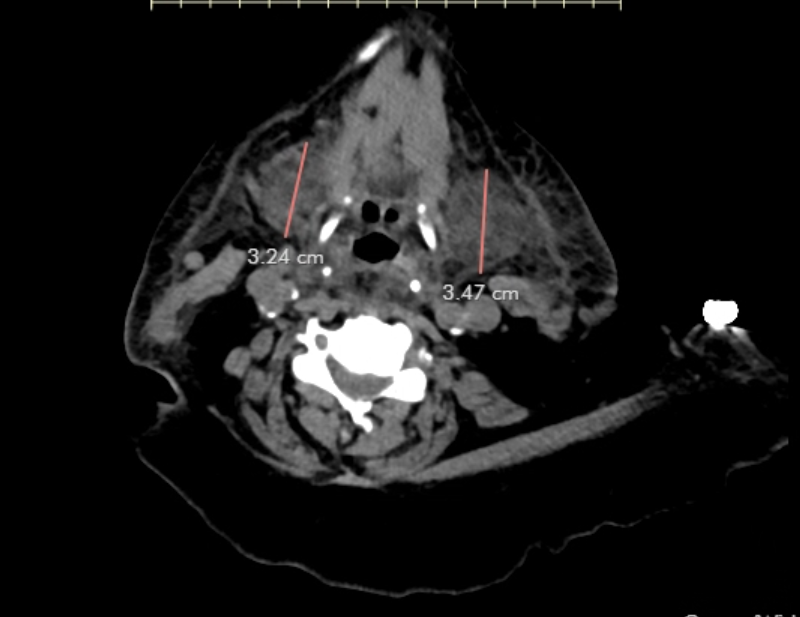
Case Presentation: A 76-year-old woman presented to the hospital with complaints of dyspnea and bilateral lower extremity edema. She had a past medical history of chronic kidney disease (CKD) stage 4 and inflammatory bowel disease with ileostomy and reported allergy to infliximab. IV furosemide was started for acute congestive heart failure. CTA chest was done (with Iopamidol 76% 100 ml), which was negative for PE.13 hours later, the patient developed neck swelling with no dysphagia or dysphonia and normal vital signs. On examination, there was neck swelling and erythema (figure 1), oropharynx was normal. A stat neck CT revealed enlarged submandibular glands (figure 2). Bilateral upper extremity doppler was negative for DVT. White blood cell count was normal. Viral serology including mumps and Epstein Barr virus antibodies were negative.Infectious disease service was consulted. Empiric antibiotics were initiated for presumed neck cellulitis.Serum iodine levels were ordered for suspected contrast induced sialadenitis, they were elevated at >100,000 ug/L. Antibiotics were discontinued. Two doses of 40 mg IV methylprednisolone were administered for management of CIS. IV fluids and non-steroidal anti-inflammatory agents were not given due to acute CHF and CKD respectively.There was a significant improvement of neck swelling the next day. Neck swelling had completely resolved at the time of discharge.
Discussion: Contrast induced sialadenitis (CIS) is an inflammatory and immunologic response. It is considered as a pseudo allergic reaction rather than a true allergy.The pathophysiology is not well understood. It is postulated to be secondary to iodine accumulation in the salivary glands causing local inflammation and edema leading to blockage of the salivary ducts. It can affect any major salivary gland but most commonly affects the submandibular glands.It may occur in patients with risk factors promoting iodine retention but has also been reported in patients with no predisposing factors. In our patient, dehydration from ileostomy output and impaired contrast clearance from underlying CKD stage 4 may be contributing factors.Serum iodine levels of >250 ug/L are associated with iodine overload. At levels >100,000 ug/L, in the appropriate clinical context, contrast-induced sialadenitis is diagnosed.No correlation has been found with this condition and prior contrast exposure. Several cases have been reported in contrast naïve patients as well as patients with previous contrast exposure. Our patient was exposed to IV contrast 7 years earlier without any reaction; she had CKD stage 3a at that time.In a meta-analysis by Jiao et al, the time of onset varied from 0.5 hours to 5 days with a mean of 30 hours.
Conclusions: The management of CIS is supportive care, with steroids playing a role in cases with a protracted clinical course. Although there have been no life-threatening reactions reported to date, this condition may reoccur and future contrast use ought to be carefully considered. Pre-treatment with steroids has shown some benefit in preventing CIS. Awareness of CIS will prevent unnecessary empiric diagnostic work-up and management.