Background: Healthcare institutions face a narrow operating budget to provide patient care. Centers for Medicare and Medicaid Services (CMS) evaluate healthcare institutions based on efficiency, quality and customer experience–in other words: length of stay, readmission rate and patients’ perception of the care they received. The effectiveness of decreased readmission is based on multiple variables, and one of the main drivers is a strong post-discharge transitional program, but how cost-effective is it to establish a transitional care program?
Purpose: To provide a well-designed transitional care program through the PDC that crosses service lines and to evaluate its impact in the rate of readmission and emergency department (ED) visits as well as cost-saving associated with this transitional program.
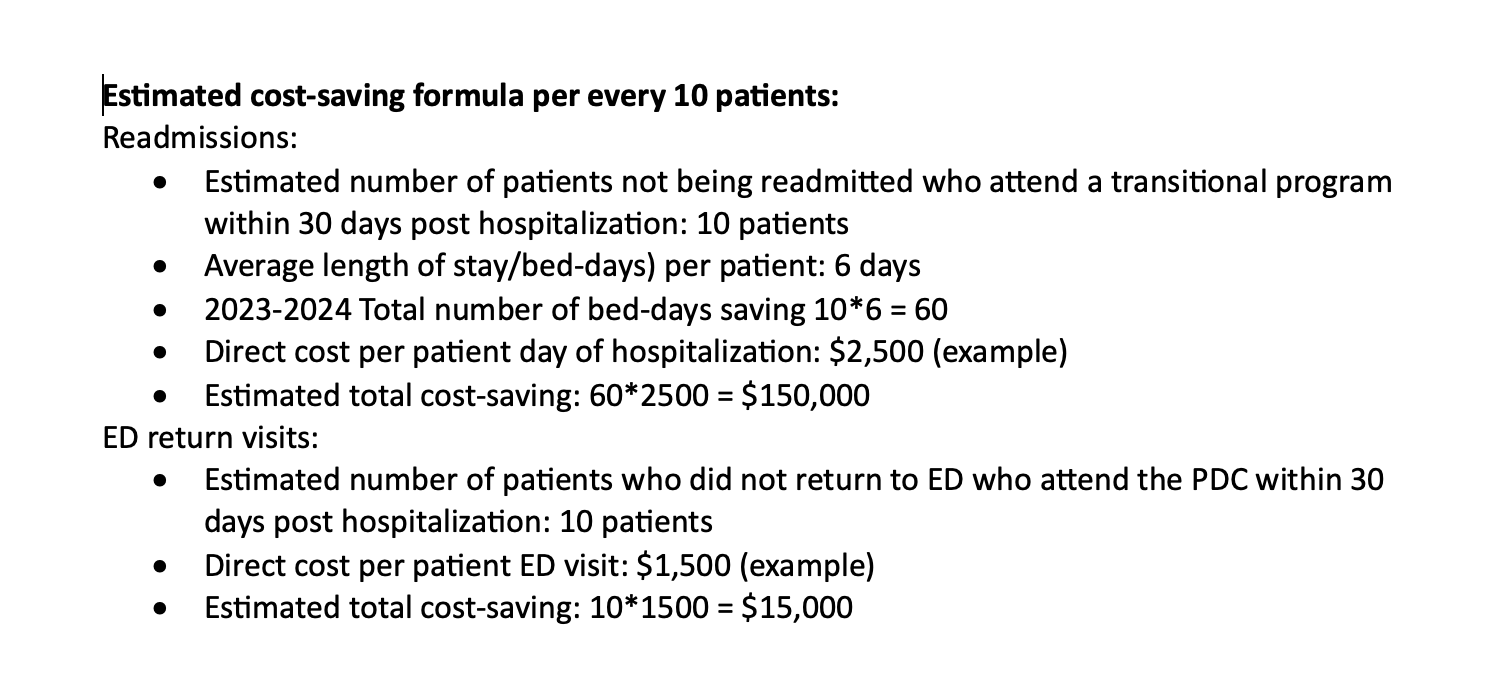
Description: We developed a post-discharge clinic (PDC) that encompasses transitional interventions for our institution without major cost based on leadership and networking with internal stakeholders. The transitional care interventions provided by the PDC were strategically designed, implemented, and iteratively evaluated–accounting for organizational goals, assessment of inpatient care processes, risk of readmission, inpatient and primary care service benchmarks, inpatient and outpatient scheduling processes, financial limitations, internal and external stakeholder input, and the diverse population seeking care at our institution. PDC has been able to expand and operate with the collaboration of hospital leadership and internal resources. Patients in the general medicine units with a higher risk of readmission who are unable to see their primary care provider (PCP) within 7 days of discharge are prioritized to be seen in the PDC. Those with lower risk of readmission are scheduled in the PDC within 14 days of discharge if they are no longer able to see their PCP. After patients are discharged from the hospital, they receive a 48-hour transitional post-discharge call. Then, during their PDC visit, patients receive comprehensive disease and medication education, medication reconciliation, opportunities to discuss any adverse events, evaluation of their social support, and referral to other services.We evaluated the cost of operations, the decrease of readmission and ED return visits, saving bed-days and cost-saving associated with the PDC interventions.QualityPatients seen at the PDC have 33% lower readmission and ED return rates in the high-risk category compared to patients not seen at the PDC. Estimation of Cost-savingThe inpatient cost-saving calculation was based on the number of patients not being readmitted (33%) who attend the PDC within 30 days post hospitalization, multiplied by the average length of stay and direct cost per patient day of hospitalization.The estimation of cost-saving in the ED was based in the number of patients who did not return to ED who attend the PDC within 30 days post hospitalization (33%) multiplied by the direct cost per patient ED visit.
Conclusions: Urgency to improve readmissions with a limited budget generates innovation to achieve goals for the organization. We achieve readmission reduction while being cost-effective. We operate without budgeted FTE but providers salaries and use of internal institutional resources. Transitional Care Management codes and new patient billing codes associated to decreased risk of readmissions shows cost-quality effectiveness for the organization