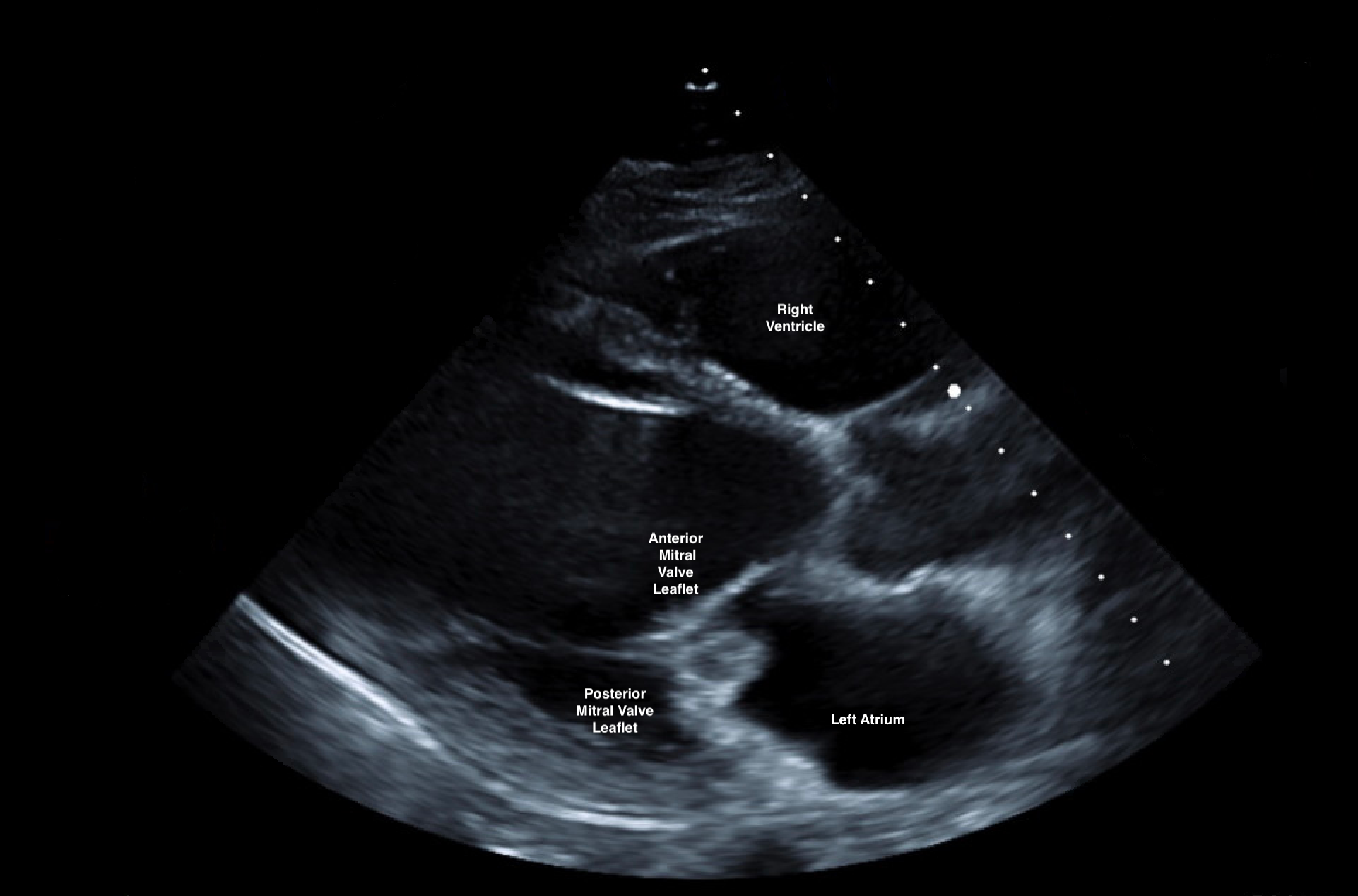
Case Presentation: A 47 year old white male with alcoholism and cirrhosis was admitted to the ICU after being found altered in his bedroom in a pool of blood draining from his nose. A rhino rocket was inserted into the patient’s right nostril to stop the bleed and labs and imaging were obtained. Labs revealed leukocytosis to 23, platelets <9, creatinine 4, lactic acid 4.1, and crp 239. The patient was pan-cultured and given fluids, platelets, vancomycin, cefepime, and eventually vasopressors. CT head revealed a left frontal hyperdense focus measuring 6 mm suspicious for subarachnoid hemorrhage. Repeat CT head showed diminishing size of the bleed eliminating the need for neurosurgical intervention. On hospital day two, the patient continued to remain altered prompting an MRI brain which revealed punctate foci suspicious for subacute lacunar infarcts raising concern for embolic phenomena. Lumbar puncture could not be performed due to persistent thrombocytopenia. Later that day, the patient desaturated and became tachypneic requiring intubation and subsequent chest x-ray revealed new moderate pulmonary edema. By this time, the patient’s blood cultures also speciated with pansusceptible Pasteurella multocida. Further history obtained from the patient’s wife revealed that the patient was scratched by an outdoor cat two weeks prior to admission. Transthoracic echocardiogram was performed and showed an irregular mass measuring 1.5 x 1.3 cm attached to the posterior leaflet of the mitral valve consistent with a vegetation. The leaflet was perforated and severe mitral regurgitation was present. Cardiothoracic surgery was consulted but declined acute surgical management due to advanced liver disease and malnutrition. The patient was treated with IV furosemide for pulmonary edema and extubated after improvement in his mental status. He is currently on treatment with ceftriaxone 2 g daily and pending further management of his mitral valve.
Discussion: P. multocida is a gram-negative coccobacillus found in the upper respiratory tract of fowl and mammals. Infections occur from dog or cat bites and cat scratches and are more common in immunocompromised hosts. Infections can be divided into three categories includingskin/soft tissue/bone, respiratory, and invasive infections including endocarditis. The treatment for endocarditis is a prolonged course of antibiotics and possible valve repair or replacement. Our patient was unique because of his development of renal failure, endocarditis with septic emboli, subarachnoid hemorrhage, and septic shock from this highly prevalent organism.
Conclusions: There have been 36 reported cases of Pasteurella endocarditis in literature to date. Thorough history and physical and a high degree of suspicion, particularly in immunocompromised hosts is necessary to prevent morbidity and mortality.