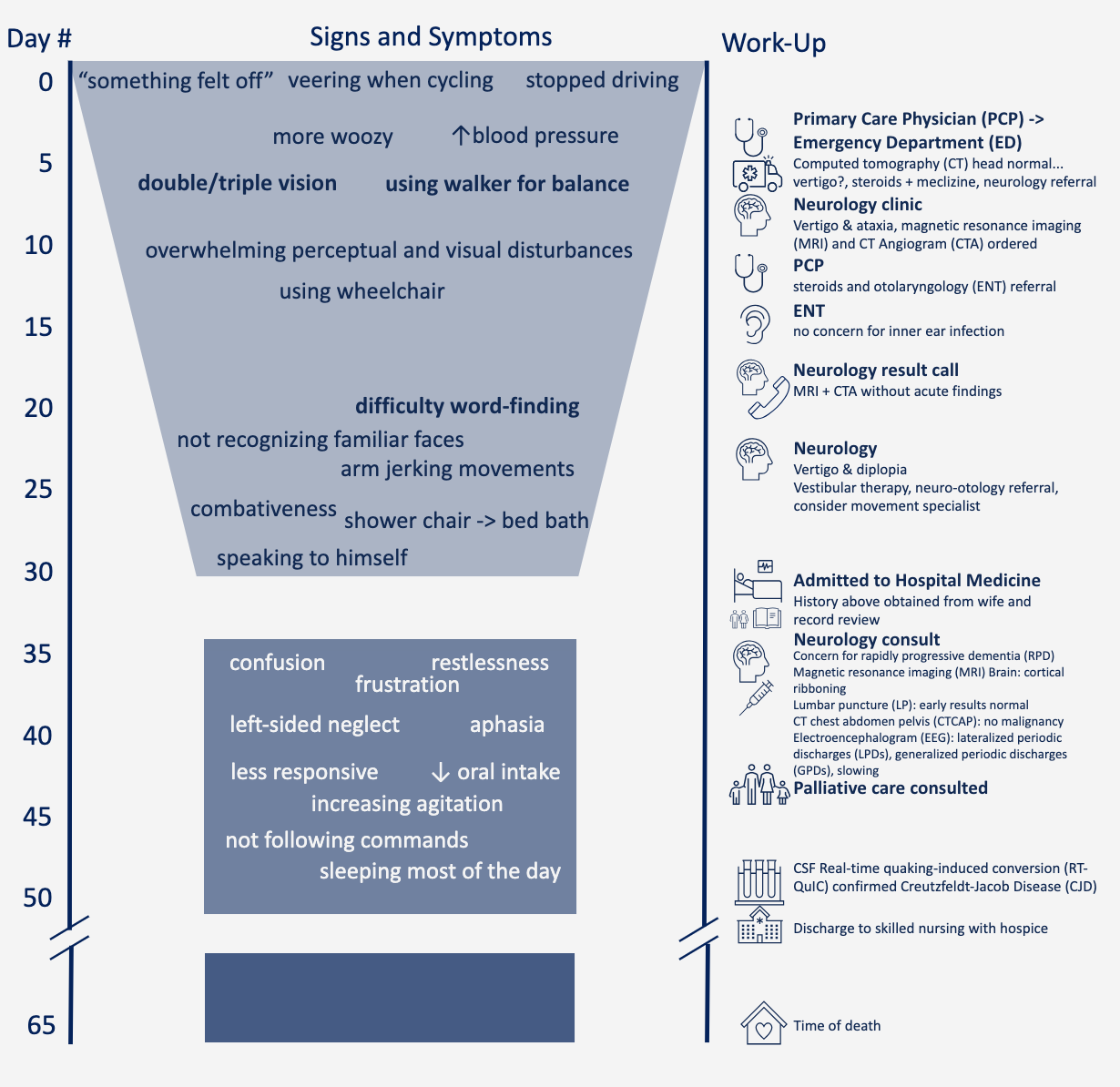
Case Presentation: Creutzfeldt-Jakob Disease (CJD) is a rare diagnosis with the global incidence estimated to be about 1-2 cases per million per year¹. Because rapidly progressive dementias (RPDs), including CJD, are rare, there is often a delay in diagnosis² which prevents preparation for end-of-life care for caregivers³. Early identification is important to help families and caregivers access appropriate resources. Here we describe a hospital presentation leading to CJD diagnosis, including interdisciplinary care while inpatient. Description: A 67-year-old previously high functioning and overall healthy man presents with a one-month history of progressive ataxia, visual changes, myoclonus, and encephalopathy. Prior to admission, his outside work-up included normal computed tomography (CT) head, magnetic resonance imaging (MRI), and CT Angiogram. Notably, he had a functional decline over 4 weeks and was dependent in his activities of daily living at the time of admission. While admitted, our patient was cared for by Hospital Medicine with initial consultation to Neurology, and eventually Palliative Medicine. Early work-up was unrevealing on extensive cerebrospinal fluid (CSF) studies, and CT chest-abdomen-pelvis was without signs of malignancy. MRI showed cortical ribboning, and electroencephalography (EEG) showed lateral periodic discharges (LPDs) and generalized periodic discharges (GPDs). Ultimately, CSF Real-time quaking-induced conversion (RT-QuIC) confirmed CJD diagnosis.
Discussion: Although our patient had a relatively typical presentation for CJD, medical work-up for his symptoms in isolation as well as a lack of familiarity with this rare diagnosis could have led to a lack of diagnostic clarity prior to admission. Early recognition of symptoms, neurology referral, and medical work-up upon hospital presentation can help to expedite diagnosis and ultimately connect patients, families, and caregivers to helpful resources such as support organizations and palliative care⁴. Additionally, provider expertise has been demonstrated to improve family and caregiver experience further emphasizing the importance of provider familiarity with this rare presentation⁵.
Conclusions: Patients with CJD will often present with cognitive difficulties, gait changes, behavioral changes, and vision concerns. Given that any of these presentations in isolation are common reasons for hospital presentation, a detailed history is important to identify and distinguish a rare presentation of RPD/CJD.