
Case Presentation:
A 71‐year‐old man was admitted to the hospital for worsening left leg cellulitis. He had noticed a “pimple” on the dorsum of his foot on Sunday. He cleaned the area with hydrogen peroxide, but the erythema spread. On Wednesday, he saw his primary care provider, who performed an incision and drainage and sent cultures. Doxycycline was initiated; however, the erythema spread with associated swelling and streaking up the leg. He was subsequently admitted to the hospital on Friday with concern for methicillin‐resistant Staphylococcus aureus (MRSA). The patient had no known trauma to the leg, no previous history of cellulitis, and no previous history of MRSA. He was healthy, with a medical history significant only for hyperlipidemia. He had an open reduction/internal fixation of his left leg in 2000 after a motor vehicle accident. He is a former smoker. He is active and frequently works out in his garden, including moving 2 truckloads of dirt 2 weeks ago. He denied tick bites or recent travel. A complete review of systems was positive for occasional joint pain and intermittent constipation. No fever, chills, night sweats, chest pains, cough, headache, or weight loss were noted. His physical exam was significant for nonpitting edema with erythema and streaking to the mid‐thigh on the left leg. There was a 1‐cm necrotic lesion on the dorsum of his foot and several nodules on the posterior aspect. His admit labs, foot x‐rays, and lower‐extremity duplex were normal. Vancomycin was initiated, with mild improvement. On Monday, the wound culture grew a few Nocardia species. Infectious diseases was consulted, which changed the antibiotics to ertapenem and trimethoprim‐sulfamethoxazole. A chest x‐ray and HIV test were negative. The patient's erythema improved dramatically, and he was discharged home a few days later on oral trimethoprim‐sulfamethoxazole for 6 months, with a final diagnosis of cutaneous nocardiosis.

Ulcerated lesion.
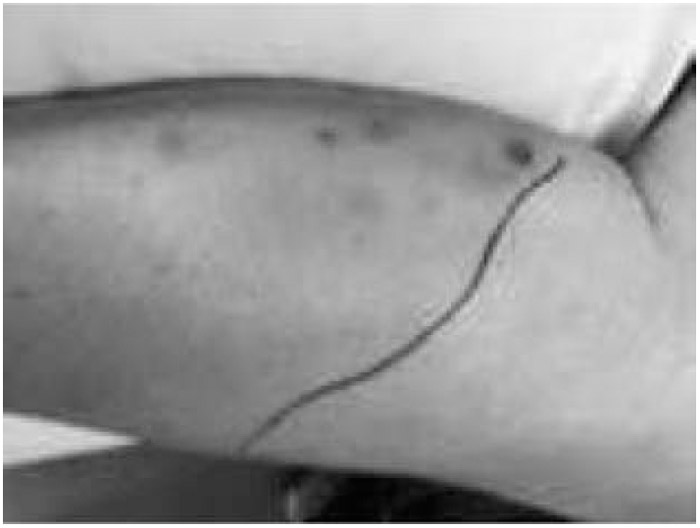
Nodular lesions with surrounding cellulitis.
Discussion:
Nocardia is a gram‐positive aerobic rod and can be identified using acid‐fast staining, or it may grow in an aerobic medium, typically taking 5–21 days. Considered an opportunistic pathogen, Nocardia typically infects immunosuppressed hosts, but approximately one third of hosts are immunocompetent. There are no specific risk factors for nocardiosis, nor does it present with pathognomonic signs or symptoms. It is classified based on location and extent of disease and includes pulmonary, central nervous system (CNS), cutaneous, and disseminated. It is found in soil worldwide, decaying vegetation, and aquatic environments and can become airborne. Inhalation is the most common mode of entry, causing aggressive infiltrates, but it may also invade via ingestion or cutaneously (as in our example). Nocardia has the ability to disseminate to most organs, with a propensity for the CNS. Despite appropriate antibiotic therapy, Nocardia can relapse or progress, making long treatment periods and careful monitoring essential.
Conclusions:
This case illustrates that cellulitis that has failed outpatient treatment is not always MRSA, and physicians need to consider other organisms.
Disclosures:
I. M. McQuistan ‐ none; S. Wenk ‐ none