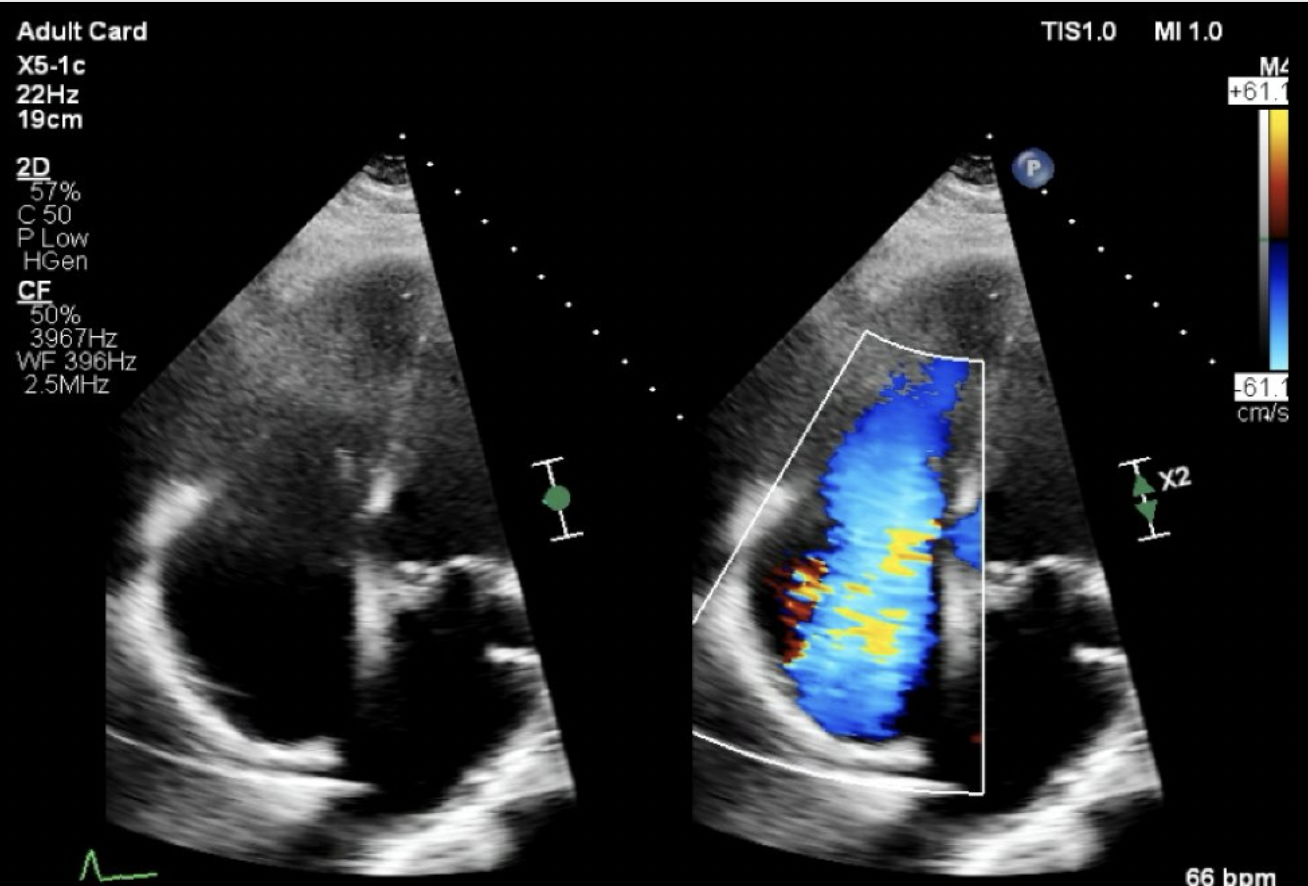
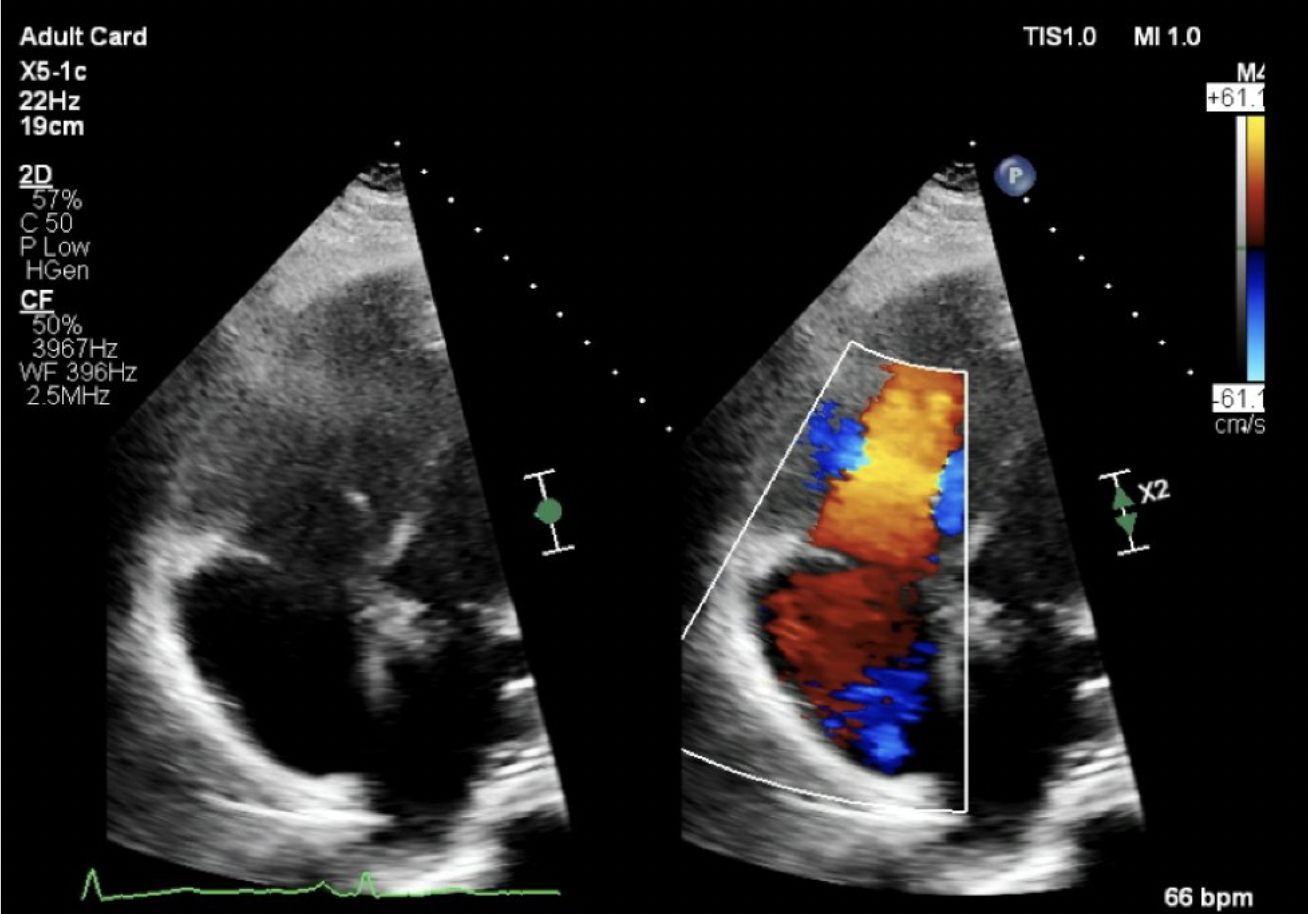
Case Presentation: A 63-year-old male with a history of carcinoid disease presented to the hospital with abdominal distention, watery diarrhea, and anasarca. His carcinoid disease was diagnosed in 2013 s/p small bowel resection with recently identified hepatic metastasis. Exam revealed facial flushing, a grade 3 systolic murmur, abdominal distension, and pitting lower extremity edema, symptoms which developed less than one year following a normal TTE. Plasma 5-HIAA level was elevated at 1719 ng/mL. TTE demonstrated an EF of 55% with paradoxical septal motion of the left ventricular segmental wall related to diastolic septal flattening from right ventricular (RV) volume overload, moderately enlarged right atria and RV, and thickened tricuspid valve leaflets. The leaflets were frozen in an open position with torrential tricuspid regurgitation and moderate to severe pulmonic regurgitation. It also revealed a patent foramen ovale (PFO). A left heart catheterization showed no ischemic disease. Cardiothoracic surgery performed tricuspid and pulmonic valve replacements and PFO closure. He was subsequently discharged with plans for monthly octreotide injections and cardiac rehabilitation.
Discussion: Carcinoid tumors are rare, only seen in 2/100,000 in the general population yearly. Cardiac involvement occurs in up to 50% of patients with known carcinoid disease, while in a minority it may be the presenting symptom, such as this patient. Carcinoid heart disease (CHD) is characterized by plaque-like deposits of fibrous tissue. CHD is an adverse prognostic indicator with manifestations primarily affecting the tricuspid valve, coronary artery vasospasm, arrhythmias, and direct myocardial tumor involvement. Previous studies have demonstrated the correlation between increased serotonin and other vasoactive mediators predisposing patients with carcinoid syndrome developing CHD. In this case, the diagnosis of recurrence was confirmed only 3 months prior to his severe heart failure, with notable changes in TTE presenting within one year. In addition, while the decreased prevalence of carcinoid syndrome limits the ability to study long term sequelae, some studies have shown that CHD typically occurs 2-5 years after initial diagnosis. Management for this condition necessitates multidisciplinary evaluation and treatment of the malignancy, surgical correction of heart failure, and optimizing medical management. Considerations for management include somatostatin analogues along with surgical replacement of TV and PV valves for definitive improvement in CHD. Otherwise, goal directed medical management is the mainstay of long-term management.
Conclusions: CHD is an adverse prognostic indicator in patients with carcinoid disease, and in the setting of severe heart failure, can be fatal. Development of cardiac sequelae can be extensive, and as seen in this case and can occur over a short period of time. It is associated with a predicted survival less than 1 year with advanced heart failure. Early detection and management is vital in improving mortality for patients presenting with this disease. In addition, CHD presenting 10 years after diagnosis is not commonly reported, likely in part due to the rare nature of the disease and thus, is difficult to study long term sequelae and requires further studies as well as multidisciplinary management.