
Background:
The discharge process is increasingly being studied as an area of quality improvement. Patients can inadvertently be discharged home with critical laboratory values or abnormal trends because of cognitive or non‐cognitive errors. Previous studies have shown that abnormal laboratory tests in the clinic and the hospital can also be lost to follow‐up, resulting in adverse events, morbidity, and mortality. It is also well known that computerized physician order entry (cPOE) programs with built‐in realtime clinical decision support systems (CDSS) can change clinical behavior and help improve patient safety.
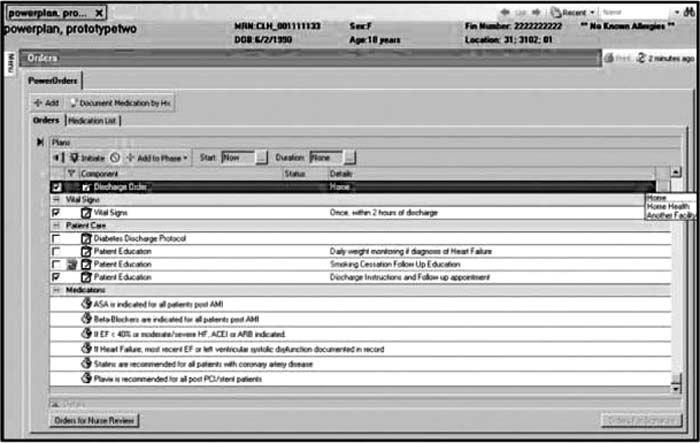
Discharge alert screen.
Purpose:
To address this problem we have created within cPOE a program with built‐in real‐time CDSS that triggers a discharge alert (DA) based on common laboratory values that are critical or trending abnormally at discharge. This DA program will trigger during the discharge process in a cPOE system if predetermined critical laboratory values or trends are exceeded in a discharged patient. The alert will then be displayed on the computer monitor during the discharge order (DO) asking the physician if he or she stills wants to proceed with discharging the patient. In this CDSS, the discharge order set needs to be checked to discharge the patient. On checking the box for the discharge order, the patients' last laboratory values (in the case of trends, difference between the last 2 values) will be screened by a computer program and the DA will be triggered if it meets any of the predetermined criteria. The physician will then have the option to proceed with the discharge or hold the discharge.
Description:
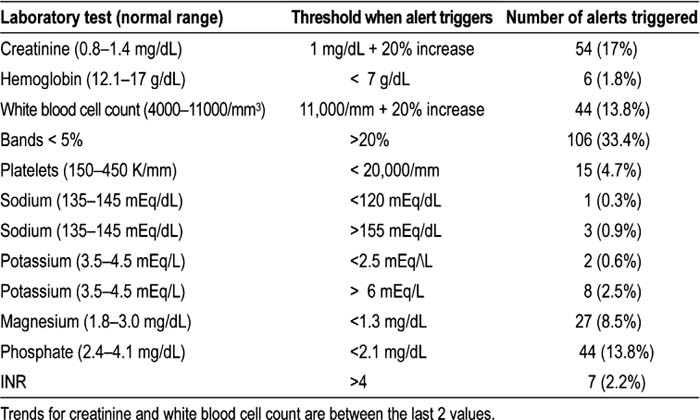
We created and tested computer rules that are based on critical laboratory values and trends in a pretest environment, and then using the data warehouse, we retrospectively looked back at all discharges in a 1‐month period in a large tertiary‐care hospitals to see how often the rules would trigger at time of discharge. In a 30‐day period there were 7955 discharges. Rules were triggered 317 times by abnormal laboratory values or trends at the time of discharge (see Table 1).
Conclusions:
A discharge alert based on rules that trigger at the time of discharge in cPOE can help to prevent the premature discharge of patients with abnormal laboratory tests. Future research should look at the refining of these rules to prevent discharge alert fatigue and at the same time act as a safety measure for the discharging physician and patient.
Author Disclosure:
G. Mathew, none; A. Kho, none; L. Huynh, none; C. Fantz, none; N. Spell, none; P. Dexter, none.