Background: Dichotomous outcomes—such as mortality—rarely capture the range of potential outcomes important to patients and clinicians. To address this limitation, the Desirability of Outcome Ranking (DOOR) score was created to rank potential outcomes from least to most desirable. Currently, there is no standardized method to develop a DOOR score and data are limited on whether patients and their clinicians rank outcomes similarly. Thus, we aimed to develop a novel DOOR score for adults hospitalized with community-acquired pneumonia (CAP) by surveying patients and clinicians on their preferred outcome ranking. Secondarily, we assessed for differences in DOOR rankings between patients and clinicians.
Methods: First, we created nine clinical scenarios describing the spectrum of potential outcomes of patients with CAP two weeks after initial emergency department visit. Cases included descriptions of persistent CAP symptoms as well as adverse side effects from antibacterial use. To ascertain clinician DOOR score, we used a snowball sampling method to recruit a target of 25 clinicians in specialties that regularly treat CAP (i.e., hospital medicine, emergency medicine, infectious diseases, pulmonology). For the patient DOOR score, we recruited patients hospitalized with CAP by reviewing electronic patient lists for adults hospitalized with pneumonia. Clinicians and patients who agreed to participate were asked to rank the 9 cases from most to least desirable in REDCap. For the patient survey, we used language reducing medical jargon. First, we used Friedman rank sum tests, to combine/collapse DOOR outcomes with scores that did not significantly differ from each other. Then, we used the Mann Whitney U test to compare DOOR rankings between physicians and patients. Final study results were presented to a national hospital medicine patient and family advisory committee (PFAC) for their impressions.
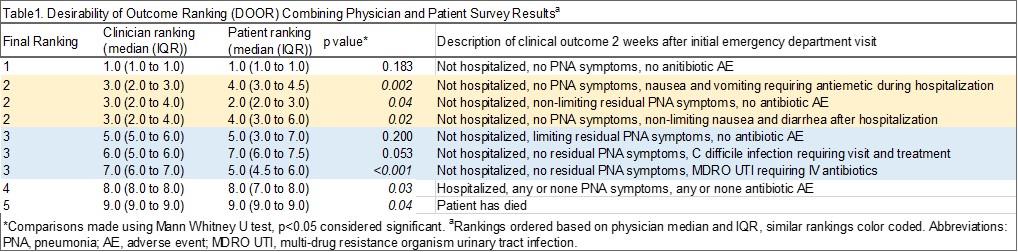
Results: We contacted a total of 31 patients and received responses from 22 patients for the DOOR survey (mean age 57.9 years). We contacted and received responses from 25 clinicians. The relative order of DOOR outcomes is shown in Table 1, separated by clinicians and patients. Combining non-significantly different DOOR outcomes resulted in collapsing of 6 cases into 2 categories for 5 overall DOOR scores that significantly differed from each other (see column 1 in Table 1 for final ranking). Notably, patients and clinicians had significantly different preferred ranking for 6 DOOR cases. Our PFAC had several hypotheses as to why clinicians and patients might have different responses (see Table 2).
Conclusions: We present a novel DOOR score derived from patient and clinician reported preferences for hospitalized adult patients with CAP. Notably, clinicians and patients differed in their perception of certain outcomes. Patients ranked symptoms that were uncomfortable but not potentially life-threatening as less desirable than physicians. Physicians tended to rank quality linked metrics such as readmission, and outcomes that significantly impact treatment courses, such as multi-drug resistant organism (MDRO) urinary tract infections (UTI), as worse than patients. When designing future trials using DOOR scores, researchers should consider including patients in DOOR score design as their perspectives may differ from clinicians.