Background: Iron deficiency is the most common cause of anemia and a common comorbidity in hospitalized patients. Iron deficiency is present in up to 50% of patients with heart failure and intravenous (IV) iron can improve symptoms, functional capacity, and quality of life1. Inflammatory bowel disease has a prevalence of iron deficiency in 25% of patients and treatment with IV iron allows for faster iron repletion and improvement in quality of life.2 Similar findings were shown in patients with malignancy, IV iron was able to decrease need for RBC transfusions.3 Additional research is active in preoperative screening for Iron deficiency and use of IV Iron to decrease perioperative transfusion requirements.
Purpose: The purpose of this work was to promote high value care with the use of intravenous iron in the inpatient setting. A knowledge gap was observed among providers regarding differences in costs and perceived risk of infusion reactions limiting the use of more cost-conscious formulations. Our goal was to increase the use of more cost effective formulations of IV iron including Iron dextran ($312), Iron sucrose ($295), and Ferric gluconate($122) as opposed to Ferumoxytol ($2,172). Prices noted are for estimated 1,000 mg dose and wholesale acquisition cost.Our preferred agent is Iron dextran with convenience of a single infusion of 1,000 mg in 1 hour with evidence for equal efficacy and safety when compared to iron sucrose and ferric carboxymaltose. 4
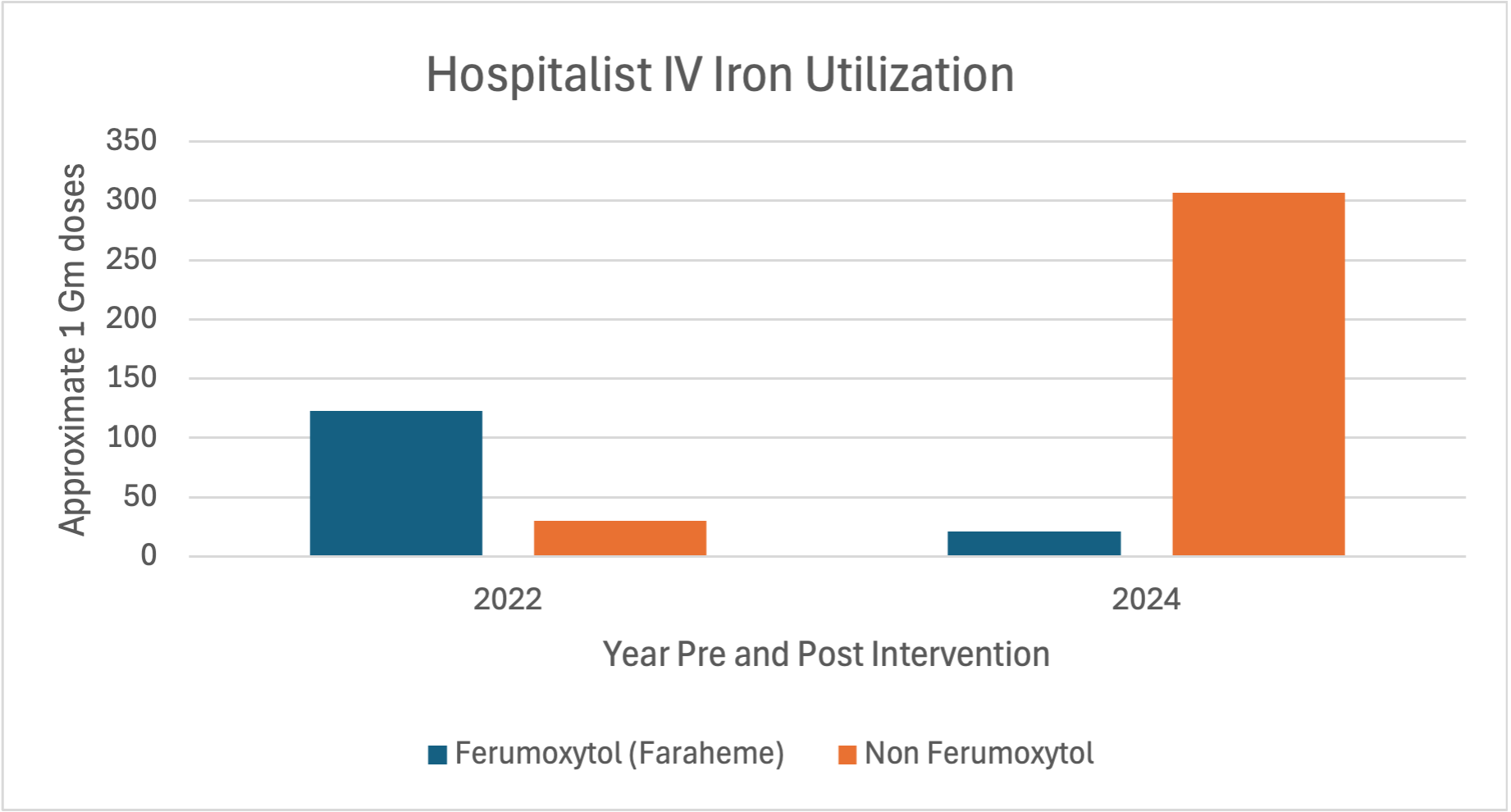
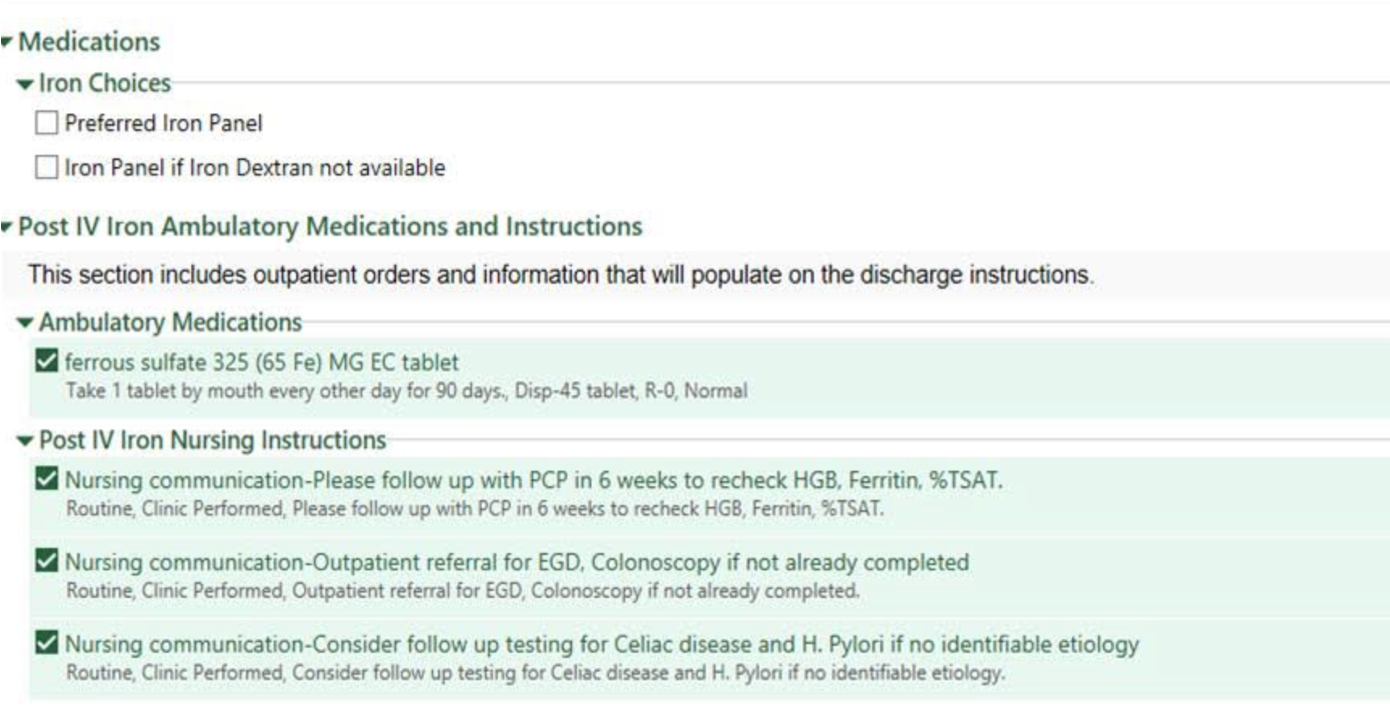
Description: We established a multidisciplinary group including hospitalists, hematology, pharmacists, and data scientists to review the treatment of iron deficiency anemia and create a comprehensive orderset in EPIC. See figure 1. The orderset includes diagnostic criteria of iron deficiency anemia with patient specific results. Iron Dextran was orderable under the preferred IV iron tab with alternatives listed under a second tab. We also included recommendations for workup of etiology and follow-up care.Our group also created a provider development session for the hospitalist group on evidence-based diagnosis and treatment of iron deficiency anemia, along with implementation of a quarterly self-review of IV iron use with individual ordering statistics.Our order set went live April 2023 with data analysis pre and post intervention.In 2022, only 19.6% (30 out of 153) orders were for the preferred non Ferumoxytol formulation. This improved dramatically in 2024 with 93.5% (307 of 328) of orders for the non Ferumoxytol one gram doses. See table 1.The use of the non Ferumoxytol formulations increased by 91% from 2022 to 2024, with conservative extrapolated cost savings of approximately $83,840 to date in 2024.
Conclusions: In conclusion, through the creation of an IV iron order set reinforced with provider education, we were able to decrease the use of the most expensive formulation of IV Iron (Ferumoxytol) by 85% with an estimated cost savings of at least $83,840 over a 1-year period among our hospitalist group. The additional benefit of this order set was also to improve diagnostic accuracy using criteria for iron deficiency incorporated into the order set and reinforce the need to consider additional evaluation for etiology, such as bidirectional endoscopy and malabsorption syndromes such as celiac disease when appropriate.