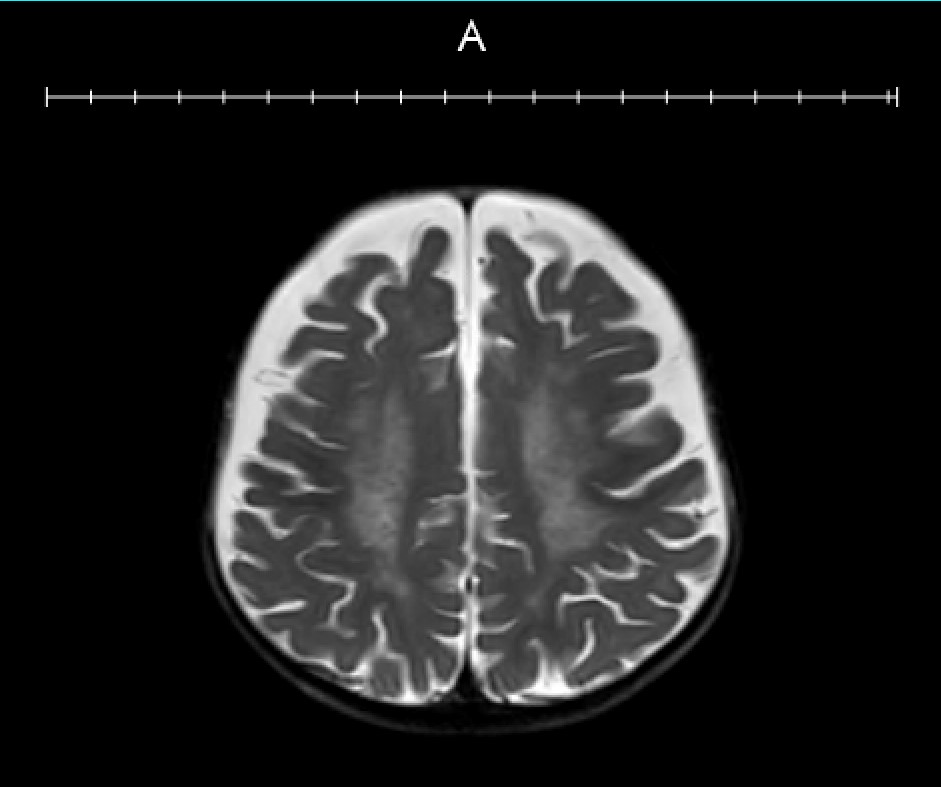
Case Presentation: A term 8-month-old infant was admitted to the hospital for concerns of inconsolable crying and diffuse hypertonicity in all four extremities. Birth history was unremarkable and newborn screens were negative. Her history was significant for loss of developmental milestones at 6-7 months of age, characterized by inability to sit without support or to track visual stimuli, and a reported decrease in height and weight to the 5th percentile. She was previously able to laugh, grab toys, and sit up.Physical exam was significant for marked irritability with hand fisting and profound hypertonia greater in the lower extremities. The patient had clonus in her bilateral lower extremities that progressed to sustained clonus during crying episodes and patellar reflexes were difficult to illicit. Extraocular movements were intact but she exhibited poor tracking. She also presented with intermittent staring spells in which she would become unresponsive to auditory and visual stimuli. Initially, the patient underwent metabolic workup with lactate, pyruvate, uric organic acids, plasma amino acids, acylcarnitine profile, and metachromatic leukodystrophy (MLD) panel, which were interpreted as normal with the exception of mildly elevated ammonia to 64.0 (nl <45). A genetic lysosomal storage disease panel was also sent out. MRI brain showed abnormal T2/FLAIR hyperintensity in a leopard skin pattern involving mostly the periventricular and deep white matter along with slight thinning of the corpus callosum.The patient was started on gabapentin and baclofen, which improved her hypertonicity and spasticity. Subsequent ophthalmologic exam and barium swallow study were unremarkable. Upon follow up, outpatient genetics testing provided confirmatory diagnosis for infantile onset Krabbe disease.
Discussion: There are four stages of infantile onset Krabbe leukodystrophy. The first stage is marked by irritability and feeding difficulties; the second stage by rapid neurological deterioration characterized by loss of developmental milestones; the third stage by sensory deficits and autonomic dysfunction; and the fourth stage by diffuse hypertonicity with eventual progression to death. Of the four stages, our patient showed features consistent with stage two, progressing to stage three.With regard to treatment options, hematopoietic stem cell (HSC) transplantation is being studied in asymptomatic patients. A recent study showed that HSC transplantation in asymptomatic infants with Krabbe leukodystrophy had improvement in receptive and expressive language, fine motor skills, adaptive behavior, and cognitive development. Our patient was evaluated for possible stem cell transplantation, however, was deemed not to be a candidate due to the advanced stage of her disease. Supportive care in the form of treating resultant issues such as seizures, spasticity or feeding difficulties is recommended for all affected patients.
Conclusions: Developmental regression is a harbinger for serious underlying disorders and always warrants a thorough workup. Among children presenting with developmental regression, mitochondrial disorders, neurometabolic disorders, and any of the thirty existing leukodystrophies are diagnoses to consider. A broad differential may also include autosomal recessive spastic ataxia of Charlevoix, Rett syndrome, and cobalamin deficiency.