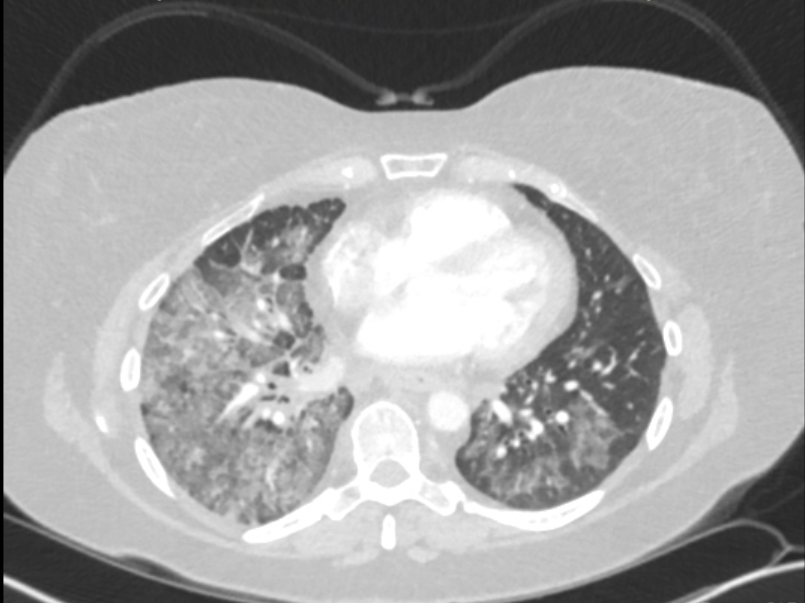
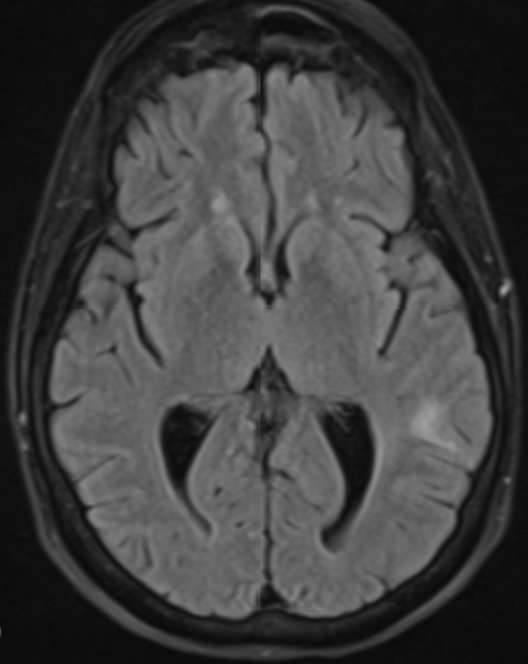
Case Presentation: A 61-year-old, non-smoking, white female with history of Coronavirus disease 2019 (COVID-19) twice, and long COVID syndrome, presented with progressively worsening dyspnea over the last five months. She was repeatedly diagnosed with pneumonia and treated with antibiotics and steroids without relief prior to hospital presentation. Workup in the hospital revealed neutrophilic leukocytosis, but no other significant findings. Computed tomography angiography of the chest led to evidence of multifocal bilateral extensive ground glass opacities with consolidation mostly in the right middle and right lower lobes, mediastinal lymphadenopathy, cervical lymphadenopathy, and left axillary lymphadenopathy. The patient was diagnosed with cryptogenic organizing pneumonia. Pulmonology was consulted who decided to perform bronchoscopy for further evaluation, but the patient was unable to tolerate laying supine without dropping oxygen saturation. Thus, conservative management was taken with broad spectrum antibiotics and steroids. Her oxygen requirements increased to 10L/min following discharge. The patient presented again to the hospital three weeks later with acute hypoxic respiratory failure after her oxygen concentrator stopped working from an electricity outage. Given recurrent dyspneic episodes now requiring high flow nasal cannula during the day and bilevel positive airway pressure at night, an in-depth infectious and autoimmune workup was performed. Consultations were made to rheumatology and infectious disease to help with diagnosis. Lab workup was negative. A repeat computed tomography (CT) of the chest was performed which again revealed diffuse bilateral ground glass opacities and mediastinal lymphadenopathy. Physical exam during this hospital encounter was notable for a palpable 1.7 cm, nontender cervical lymph node. She subsequently underwent ultrasound guided lymph node biopsy for further evaluation. Pathology revealed metastatic adenocarcinoma of pulmonary origin. Brain magnetic resonance imaging was performed and revealed at least 8 brain metastases involving the parietal, frontal, temporal lobes, and cerebellum. Additionally, CT of the abdomen revealed a 1.7 cm hypodense lesion in the right hepatic lobe. Overall impression was that of stage IVB T2-3 N3 M1B non-small cell lung cancer, adenocarcinoma subtype.
Discussion: This case was a diagnostic dilemma given that the patient had a history of COVID-19, which can radiologically present similarly to adenocarcinoma of the lung. Bilateral ground glass opacities in the lung peripheries are the identifying feature of these pathologies (1,2,3). There was a delay in accurate diagnosis since the patient could not tolerate bronchoscopy and she initially did not present with palpable lymphadenopathy amenable to biopsy. Additionally, she did not display clinical signs or symptoms of metastatic brain disease including fatigue, focal neurological deficits, seizure, or syncope. The patient’s recurrent cough and respiratory failure were attributed to pneumonia.
Conclusions: Given the similar radiologic appearance of COVID-19 pneumonia, and adenocarcinoma of the lung, extra care should be taken to rule out lung cancer in patients who have a history of COVID-19 and present with recurrent respiratory failure. Accurate and timely diagnosis of metastatic adenocarcinoma could have prevented excess use of antibiotics and steroids, increased oxygen requirements, and repeated hospital admissions in this case.