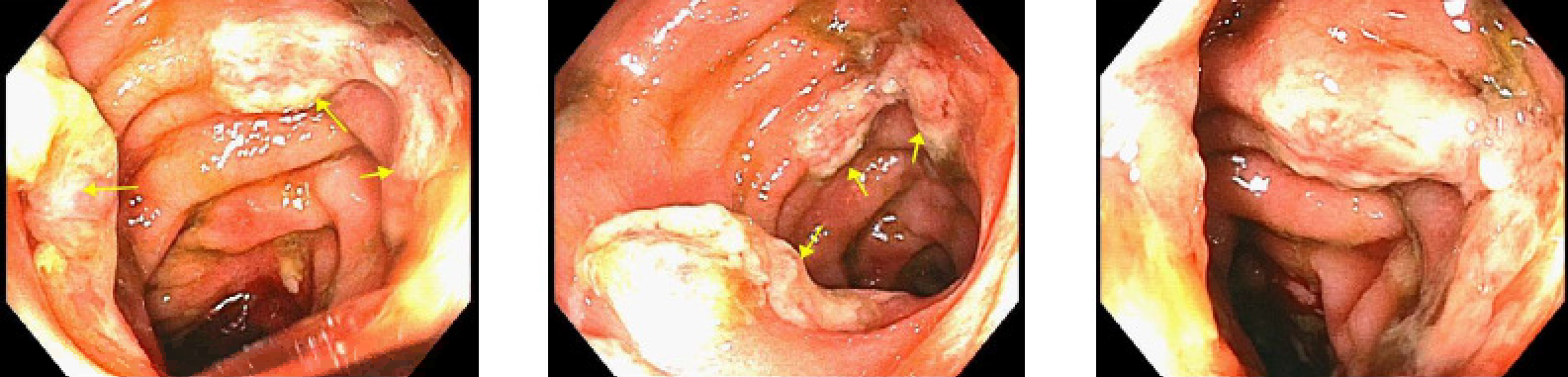
Case Presentation: A 53 year old female with history of myelodysplastic syndrome with reduced intensity conditioning bone marrow transplant (43 days prior) presented to the bone marrow clinic with several days of worsening diarrhea. She was directly admitted due to concern for graft versus host disease (GVHD). She underwent flexible sigmoidoscopy and was found to have congestion, erosions, erythema, and deep ulcerations in the sigmoid colon. Biopsies were obtained, with pathology consistent with acute GVHD. She was started on budesonide, octreotide, and total parenteral nutrition. Due to severe diarrhea, ruxolitinib and basiliximab were added. With lack of improvement, the patient was considered to have steroid refractory GVHD. Her steroids were decreased and she began extracorporeal photopheresis. Hospital course was complicated by CMV pneumonitis, CMV viremia, and hypovolemic shock. The patient continued to have significant stool output. One month into her admission, she developed aspiration pneumonia requiring intubation. Family later made the decision to transition to comfort care.
Discussion: Diarrhea is a common problem in hospitalized patients, and workup is important as it can sometimes be the presentation of a serious complication of another syndrome. Acute GVHD is a complication of hematopoietic cell transplants that can affect the skin, gastrointestinal tract, and liver. It is diagnosed by abdominal cramps, diarrhea, rash, and elevation of serum bilirubin within the first 100 days post-transplant. GVHD is staged from I to IV, with stage I requiring topical treatment as well as prophylaxis and stage II or greater requiring initiation of systemic glucocorticoids. In patients with gastrointestinal involvement, it is recommended to confirm the diagnosis with tissue evaluation and initiate nonabsorbable oral steroids as local therapy. Response to glucocorticoids is seen in less than 50% of patients, and those who lack response have high morbidity and mortality. Steroid resistance is thought to be caused by therapy failure alone, destruction of intestinal mucosa, and/or coexistence of intestinal infection. For those with steroid refractory GVHD, second line therapies such as monoclonal or polyclonal antibodies and extracorporeal photopheresis are necessary. At this time, there is limited data to help guide therapy choice. If first line treatment fails, repeat endoscopy and biopsy should be considered, as well as testing for infections within the gastrointestinal tract. Ultimately, patients with steroid refractory GVHD have increased risk for infection, which contributes to mortality rates in excess of 90%.
Conclusions: Acute GVHD is a complication of hematopoietic cell transplants that has high morbidity and mortality and typically presents as severe diarrhea. First line treatment with corticosteroids should be initiated promptly, with subsequent tissue evaluation, screening for infection, and interval determination for need to begin second line therapies.