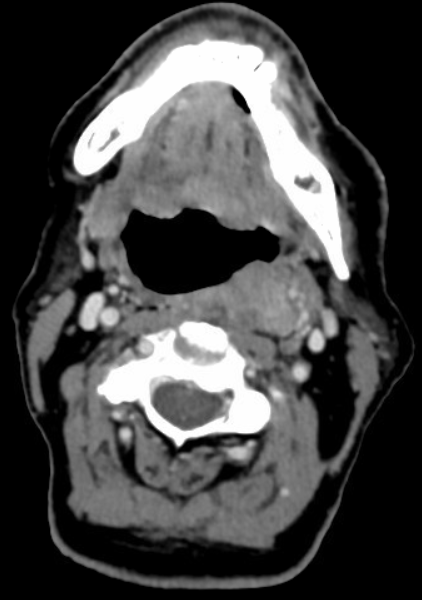
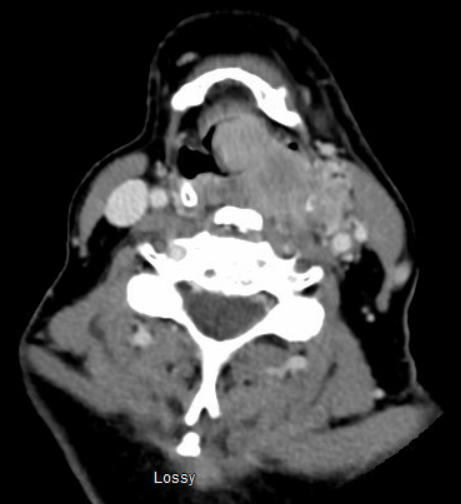
Case Presentation: 70-year-old male with a history of prior renal cell carcinoma, type 2 diabetes, CKD, and s/p nephrectomy was evaluated in an outside emergency department three times in one month for neck pain, fatigue, hypotension, and unexplained weight loss. However, his most recent visit included fevers and worsening muffled voice for 3 days. His exam was pertinent for cervical lymphadenopathy, tachycardia, and mild tonsillar edema bilaterally without signs of infection. CBC showed no signs of leukocytosis but did have mild lymphocytopenia. BMP showed hypercalcemia, trending upward since his last two ER visits. TSH was normal, and viral testing for COVID-19 and Influenza was negative. Computed Tomography of his neck soft tissue revealed a large mass in the posterior left oropharynx extending anteriorly and through the flat planes and epiglottis, concerning for malignancy. Patient was taken to the OR the following day for tracheostomy and biopsy of the mass. Tissue pathology confirmed metastatic renal cell carcinoma that stained positive for CD10, PAX8, and CKWSS with a high proliferative index. He was discharged on POD 15 with complications of atrial fibrillation and hyponatremia, and with planned oncology follow-up for radiation therapy.
Discussion: Renal cell carcinoma (RCC) constitutes roughly 3% of adult cancers and most commonly occurs in patients between the ages of 60 and 70 (1). RCC metastases in the head and neck are uncommon compared to the bones, brain, or liver, and constitutes roughly 15% of overall metastases (2). Furthermore, tonsillar metastases have only been recorded in six prior cases (3). Grange et al reported that RCC metastases spread via microvesicles in hematogenous settings, with the immune system appearing to play an important role as well (4). Treatment of RCC can involve radical nephrectomy as is the case with our patient described above, however the prevalence of metastases s/p nephrectomy occurs in 7-30% of patients in the first five years (5). Previous treatment of tonsillar metastases was heavily debated, largely due to its low prevalence and evidence that RCC was radioresistant, leading to more surgical intervention (3). However, given more cases of atypical metastasis several years after initial diagnosis or nephrectomy have occurred, this provides an opportunity for new ablative therapies to tackle metastatic tumors and initiate local control (6,7). One of these treatments involves using stereostatic radiation therapy for either curative or palliative care (8). In the case with our patient, he is schedule to undergo stereostatic radiation therapy over the course of 5 treatments, with CT simulation for pre-treatment radiation planning.
Conclusions: Metastases to the tonsils should be considered in patients with previous renal cell carcinoma despite radical nephrectomy treatment. The current course of surgical excision versus radiotherapy should be explored further in patient management.