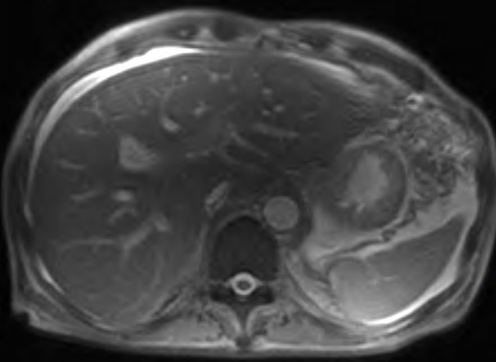
Case Presentation: 61 year old Hispanic male with a history of end-stage renal disease receiving scheduled hemodialysis, type 2 diabetes presented with 2 months of progressive abdominal pain and distension, anorexia, and intermittent fevers. He had lived in Fresno, Ca for over 20 years. Five months prior, he was diagnosed and treated for COVID-19 pneumonia. Physical exam is notable for abdominal distension with diffuse tenderness. Labs showed WBC count 14,900 with significant elevated alkaline phosphatase was 1434 and mild elevation of ALT and AST, 133 and 176 respectively. CA 19-9 was 31 and CEA was 2.3, both within normal limits. HIV screening was non-reactive. CT abdomen and pelvis shows large amounts of ascites (Figure 1) with small right pleural effusion and several lung base nodules. MRI of the abdomen with gadoterate again demonstrated perihepatic, pericholecystic, and perisplenic ascites (Figure 2). Abdominal paracentesis was performed and fluid analysis revealed WBC of 733 with 97% lymphocyte, 1% segmented neutrophil, and 2% monocyte histiocyte. Gram stain and ascites fluid culture did not reveal any organism. Given unexplained ascites and pulmonary nodules, acid fast bacilli stain and culture obtained however revealed no growth. Coccidioides antibody IgG and IgM positive with coccidioidomycosis complement fixation titer being 1:256, indicating disseminated coccidioidomycosis. Patient was started and maintained on oral Fluconazole. 3 weeks after initiation of antifungal therapy, ascitic fluid amount has significantly diminished and patient remains afebrile with improved appetite and mood.
Discussion: New onset ascites typically point towards portal hypertension, nephrotic syndrome, malnutrition or cancer. Of all the individuals who become exposed to Coccidioides immitis, only about approximately 40% become symptomatic with the symptoms being mainly limited to the lungs. Only less than 1% develop widespread disseminated infection (3). Peritoneal coccidioidomycosis can clinically present in a variety of ways ranging from an incidentally found asymptomatic indolent disease to a full-blown acute abdominal process with peritoneal irritation and ascites (4). Azole medication are considered first line treatment in various form of Coccidioides infection.
Conclusions: Coccidiomycosis masquerading as lung cancer in the form of pulmonary nodules are widely mentioned in the literature. This is a rare case of Intra-abdominal coccidioidomycosis, even in endemic areas which are presented with ascites as the only apparent clinical manifestation. It is imperative for Healthcare providers to be aware of this rare presentation to avoid misdiagnosis and unnecessary testing. Fluconazole (azole antifungal medications) is considered to be a first line agent for treatment.